

Comparing Efficacy of Preoperative neo-Adjuvant Chemotherapy and Surgery versus Surgery Alone in Patients with Resectable Gastroesophageal Cancer
- PMID: 24505539
- PMCID: PMC3915424
Comparing Efficacy of Preoperative neo-Adjuvant Chemotherapy and Surgery versus Surgery Alone in Patients with Resectable Gastroesophageal Cancer
Abstract
Background: Recent researches have led to find strategies to prevent relapse and to improve survival for gastric cancer patients, including preoperative neo-adjuvant approaches. However, the efficacy of some neo-adjuvant regimens including 5-fluorouracil, cisplatin, and docetaxel have been less investigated. The present study evaluated the outcome and mid-term survival of patients with gastric cancer who undergoing this regimen.
Methods: In a randomized double-blinded controlled trial performed at the Firoozgar hospital in Tehran in 2011-12, 61 patients were randomly assigned to treatment (32 to neo-adjuvant chemotherapy with docetaxel, cisplatin and 5-fluorouracil (5-FU) before surgery and 27 to surgery alone). The present study tried to assess the efficacy of neoadjuvant chemotherapy regarding improvement of mid-term survival, complications, and R0 resection status.
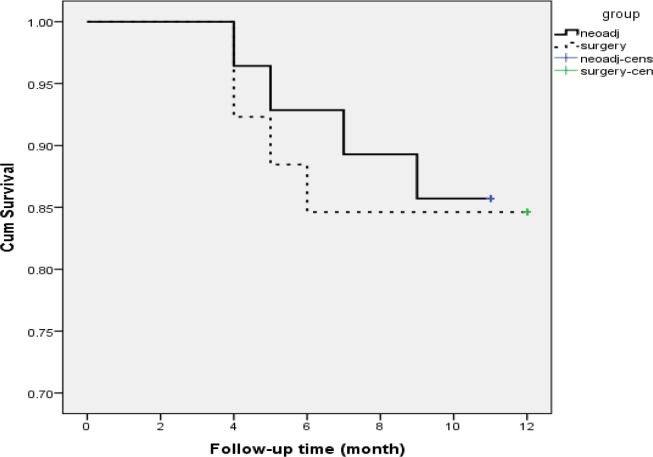
Results: The two groups were matched in terms of gender, mean age, cancer location, and TNM staging. However, R0 resection in the former group was 85.7%; while this indicator in the isolated surgery group was significantly lower (61.5%). Regarding WHO performance, no significant difference was observed across the two groups. Patients in neo-adjuvant chemotherapy group were followed for mean follow-up time 10.32 months and those who categorized in isolated surgery group were followed for mean follow-up time 10.88 months. Mid-term mortality rate in the two groups was 14.3% and 15.4%, respectively (p = 0.866). In this regard, 3-, 6-, and 9-month survival rate in neo-adjuvant chemotherapy group was 96.4%, 89.3%, and 85.7%, respectively. These survival rates in the surgery group were 92.3%, 88.5%, and 84.6%, respectively. Multivariable logistic regression analysis showed that among all study variables, only R0 resection status could predict mid-term mortality.
Conclusion: Neo-adjuvant chemotherapy and surgery compare to surgery alone more improve R0 resection status, but mid-term survival rate is similar in the two regiments. R0 resection status can effectively predict appropriate mid-term survival in undertreated patients.
Keywords: Chemotherapy; Gastroesophageal junction; Mortality; Surgery.
Figures
References
-
- Parkin DM. Global cancer statistics in the year 2000. Lancet Oncol. 2001;2:533–543. - PubMed
-
- Levi F, Lucchini F, Negri E, et al. Cancer mortality in Europe, 1995–1999, and an overview of trends since 1960. Int J Cancer. 2004;110:155–169. - PubMed
-
- Levi F, Lucchini F, Gonzalez JR, et al. Monitoring falls in gastric cancer mortality in Europe. Ann Oncol. 2004;15:338–345. - PubMed
-
- Engstrom PF, Lavin DT, Douglass HO, Brunner KW. Postoperative adjuvant 5-fluorouracil plus methyl-CCNU therapy for gastric cancer patients. Eastern Cooperative Oncology Group (EST 3275) Cancer. 1985;55:1868–1873. - PubMed
-
- Coombes RC, Schein PS, Chilvers CED, et al. A randomized trial comparing adjuvant fluorouracil, doxorubicin and mitomycin with no treatment in operable gastric cancer. J Clin Oncol. 1990;8:1362–1369. - PubMed
LinkOut - more resources
Full Text Sources