

Efficacy and safety of rifampicin for multiple system atrophy: a randomised, double-blind, placebo-controlled trial
- PMID: 24507091
- PMCID: PMC4030757
- DOI: 10.1016/S1474-4422(13)70301-6
Efficacy and safety of rifampicin for multiple system atrophy: a randomised, double-blind, placebo-controlled trial
Abstract
Background: No available treatments slow or halt progression of multiple system atrophy, which is a rare, progressive, fatal neurological disorder. In a mouse model of multiple system atrophy, rifampicin inhibited formation of α-synuclein fibrils, the neuropathological hallmark of the disease. We aimed to assess the safety and efficacy of rifampicin in patients with multiple system atrophy.
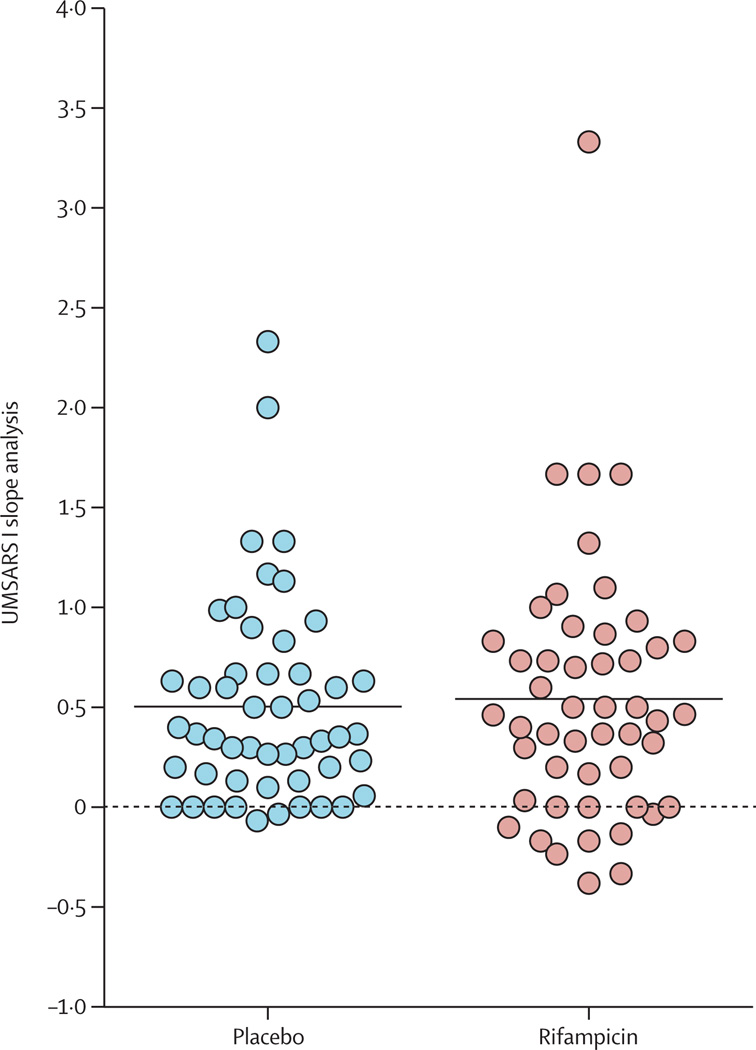
Methods: In this randomised, double-blind, placebo-controlled trial we recruited participants aged 30-80 years with possible or probable multiple system atrophy from ten US medical centres. Eligible participants were randomly assigned (1:1) via computer-generated permuted block randomisation to rifampicin 300 mg twice daily or matching placebo (50 mg riboflavin capsules), stratified by subtype (parkinsonian vs cerebellar), with a block size of four. The primary outcome was rate of change (slope analysis) from baseline to 12 months in Unified Multiple System Atrophy Rating Scale (UMSARS) I score, analysed in all participants with at least one post-baseline measurement. This study is registered with ClinicalTrials.gov, number NCT01287221.
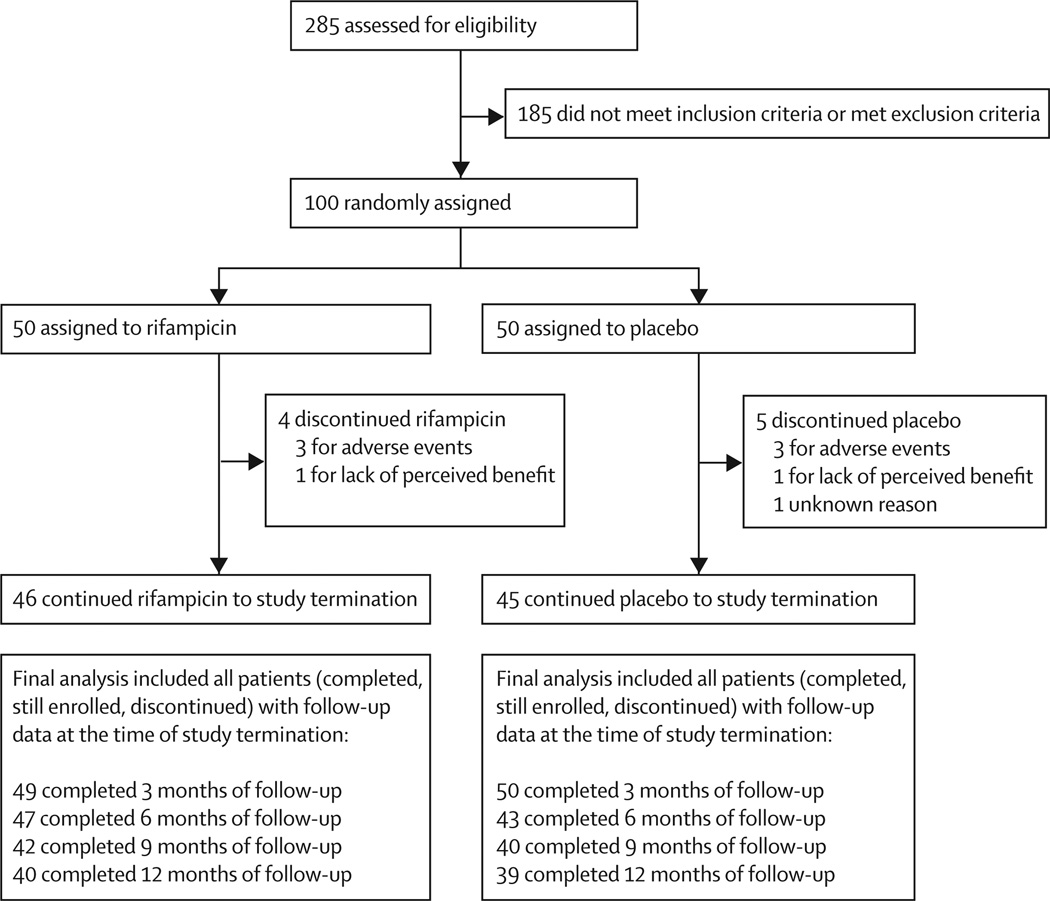
Findings: Between April 22, 2011, and April 19, 2012, we randomly assigned 100 participants (50 to rifampicin and 50 to placebo). Four participants in the rifampicin group and five in the placebo group withdrew from study prematurely. Results of the preplanned interim analysis (n=15 in each group) of the primary endpoint showed that futility criteria had been met, and the trial was stopped (the mean rate of change [slope analysis] of UMSARS I score was 0.62 points [SD 0.85] per month in the rifampicin group vs 0.47 points [0.48] per month in the placebo group; futility p=0.032; efficacy p=0.76). At the time of study termination, 49 participants in the rifampicin group and 50 in the placebo group had follow-up data and were included in the final analysis. The primary endpoint was 0.5 points (SD 0.7) per month for rifampicin and 0.5 points (0.5) per month for placebo (difference 0.0, 95% CI -0.24 to 0.24; p=0.82). Three (6%) of 50 participants in the rifampicin group and 12 (24%) of 50 in the placebo group had one or more serious adverse events; none was thought to be related to treatment.
Interpretation: Our results show that rifampicin does not slow or halt progression of multiple system atrophy. Despite the negative result, the trial does provide information that could be useful in the design of future studies assessing potential disease modifying therapies in patients with multiple system atrophy.
Funding: National Institutes of Health, Mayo Clinic Center for Translational Science Activities, and Mayo Funds.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Conflict of interest statement
We declare that we have no conflicts of interest.
Figures
Comment in
-
Rifampicin for multiple system atrophy.Lancet Neurol. 2014 Mar;13(3):237-9. doi: 10.1016/S1474-4422(14)70022-5. Epub 2014 Feb 5. Lancet Neurol. 2014. PMID: 24507092 Free PMC article. No abstract available.
References
-
- Wakabayashi K, Takahashi H. Cellular pathology in multiple system atrophy. Neuropathology. 2006;26:338–345. - PubMed
-
- Benarroch EE, Schmeichel AM, Parisi JE. Depletion of mesopontine cholinergic and sparing of raphe neurons in multiple system atrophy. Neurology. 2002;59:944–946. - PubMed
-
- Benarroch EE, Schmeichel AM, Sandroni P, Low PA, Parisi JE. Differential involvement of hypothalamic vasopressin neurons in multiple system atrophy. Brain. 2006;129:2688–2696. - PubMed
-
- Yoshida M. Multiple system atrophy: alpha-synuclein and neuronal degeneration. Neuropathology. 2007;27:484–493. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
