

Framingham score and LV mass predict events in young adults: CARDIA study
- PMID: 24507735
- PMCID: PMC4068332
- DOI: 10.1016/j.ijcard.2014.01.003
Framingham score and LV mass predict events in young adults: CARDIA study
Abstract
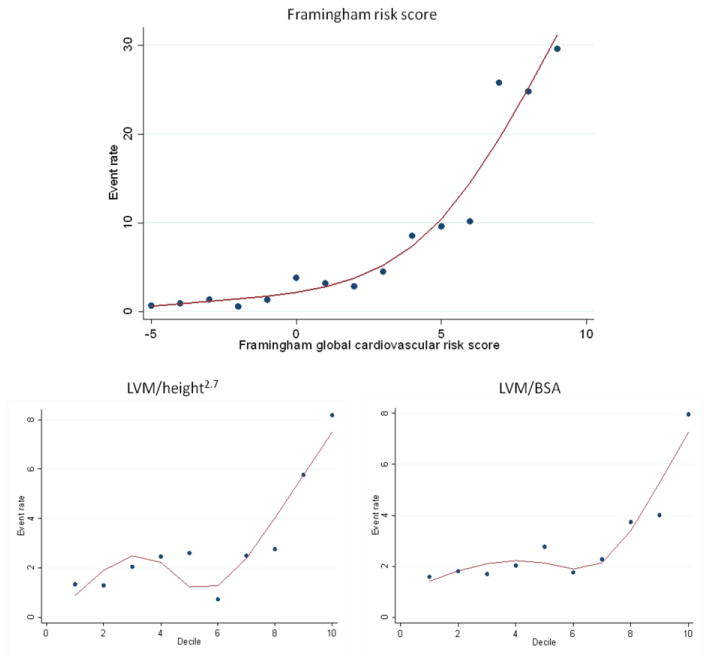
Background: Framingham risk score (FRS) underestimates risk in young adults. Left ventricular mass (LVM) relates to cardiovascular disease (CVD), with unclear value in youth. In a young biracial cohort, we investigate how FRS predicts CVD over 20 years and the incremental value of LVM. We also explore the predictive ability of different cut-points for hypertrophy.
Methods: We assessed FRS and echocardiography-derived LVM (indexed by body surface area or height2.7) from 3980 African-American and white Coronary Artery Risk Development in Young Adults (CARDIA) participants (1990-1991); and followed over 20 years for a combined endpoint: cardiovascular death; nonfatal myocardial infarction, heart failure, cerebrovascular disease, and peripheral artery disease. We assessed the predictive ability of FRS for CVD and also calibration, discrimination, and net reclassification improvement for adding LVM to FRS.
Results: Mean age was 30±4 years, 46% males, and 52% white. Event incidence (n=118) across FRS groups was, respectively, 1.3%, 5.4%, and 23.1% (p<0.001); and was 1.4%, 1.3%, 3.7%, and 5.4% (p<0.001) across quartiles of LVM (cut-points 117 g, 144 g, and 176 g). LVM predicted CVD independently of FRS, with the best performance in normal weight participants. Adding LVM to FRS modestly increased discrimination and had a statistically significant reclassification. The 85th percentile (≥116 g/m2 for men; ≥96 g/m2 for women) showed event prediction more robust than currently recommended cut-points for hypertrophy.
Conclusion: In a biracial cohort of young adults, FRS and LVM are helpful independent predictors of CVD. LVM can modestly improve discrimination and reclassify participants beyond FRS. Currently recommended cut-points for hypertrophy may be too high for young adults.
Keywords: Cardiovascular risk; Echocardiography; Left ventricular hypertrophy; Young adults.
Copyright © 2014 Elsevier Ireland Ltd. All rights reserved.
Figures
References
-
- D'Agostino RB, Sr, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008 Feb 12;117(6):743–753. - PubMed
-
- Greenland P, Alpert JS, Beller GA, et al. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2010 Dec 21;122(25):e584–636. - PubMed
-
- Marma AK, Lloyd-Jones DM. Systematic examination of the updated Framingham heart study general cardiovascular risk profile. Circulation. 2009 Aug 4;120(5):384–390. - PubMed
-
- Mancia G, De Backer G, Dominiczak A, et al. 2007 Guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) Eur Heart J. 2007 Jun;28(12):1462–1536. - PubMed
-
- The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004 Aug;114(2 Suppl 4th Report):555–576. - PubMed
Publication types
MeSH terms
Grants and funding
- N01 HC095095/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- P30 DK079626/DK/NIDDK NIH HHS/United States
- N01-HC-95095/HC/NHLBI NIH HHS/United States
- N01-HC-48050/HC/NHLBI NIH HHS/United States
- N01-HC-48049/HC/NHLBI NIH HHS/United States
- N01 HC045134/HC/NHLBI NIH HHS/United States
- N01 HC048047/HL/NHLBI NIH HHS/United States
- N01 HC048050/HL/NHLBI NIH HHS/United States
- N01-HC-48048/HC/NHLBI NIH HHS/United States
- N01-HC-48047/HC/NHLBI NIH HHS/United States
- NHLBI-HC-09-08/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
