

Metal chelator combined with permeability enhancer ameliorates oxidative stress-associated neurodegeneration in rat eyes with elevated intraocular pressure
- PMID: 24509160
- PMCID: PMC4005814
- DOI: 10.1016/j.freeradbiomed.2014.01.039
Metal chelator combined with permeability enhancer ameliorates oxidative stress-associated neurodegeneration in rat eyes with elevated intraocular pressure
Abstract
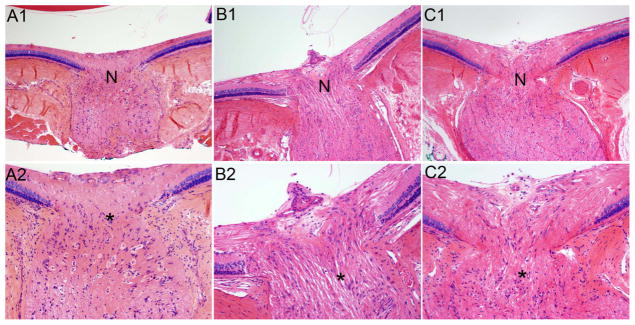
Because as many as half of glaucoma patients on intraocular pressure (IOP)-lowering therapy continue to experience optic nerve toxicity, it is imperative to find other effective therapies. Iron and calcium ions play key roles in oxidative stress, a hallmark of glaucoma. Therefore, we tested metal chelation by means of ethylenediaminetetraacetic acid (EDTA) combined with the permeability enhancer methylsulfonylmethane (MSM) applied topically on the eye to determine if this noninvasive treatment is neuroprotective in rat optic nerve and retinal ganglion cells exposed to oxidative stress induced by elevated IOP. Hyaluronic acid (HA) was injected into the anterior chamber of the rat eye to elevate the IOP. EDTA-MSM was applied topically to the eye for 3 months. Eyeballs and optic nerves were processed for histological assessment of cytoarchitecture. Protein-lipid aldehyde adducts and cyclooxygenase-2 (COX-2) were detected immunohistochemically. HA administration increased IOP and associated oxidative stress and inflammation. Elevated IOP was not affected by EDTA-MSM treatment. However, oxidative damage and inflammation were ameliorated as reflected by a decrease in formation of protein-lipid aldehyde adducts and COX-2 expression, respectively. Furthermore, EDTA-MSM treatment increased retinal ganglion cell survival and decreased demyelination of optic nerve compared with untreated eyes. Chelation treatment with EDTA-MSM ameliorates sequelae of IOP-induced toxicity without affecting IOP. Because most current therapies aim at reducing IOP and damage occurs even in the absence of elevated IOP, EDTA-MSM has the potential to work in conjunction with pressure-reducing therapies to alleviate damage to the optic nerve and retinal ganglion cells.
Keywords: Chelation therapy; EDTA; Free radicals; Glaucoma; Glaucomatous neurodegeneration; Hyaluronic acid; Inflammation; Intraocular pressure; Metal chelation; Methylsulfonylmethane; Ocular hypertension; Oxidative damage; Oxidative stress; Reactive oxygen species; Retinal ganglion cell.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures









References
-
- Halliwell B. Reactive oxygen species and the central nervous system. J Neurochem. 1992;59:1609–1623. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
