

Yield of downstream tests after exercise treadmill testing: a prospective cohort study
- PMID: 24509269
- PMCID: PMC4033667
- DOI: 10.1016/j.jacc.2013.11.052
Yield of downstream tests after exercise treadmill testing: a prospective cohort study
Abstract
Objectives: The purpose of this study was to estimate the frequency and results of downstream testing after exercise treadmill tests (ETTs).
Background: The utility of additional diagnostic testing after ETT is not well characterized.
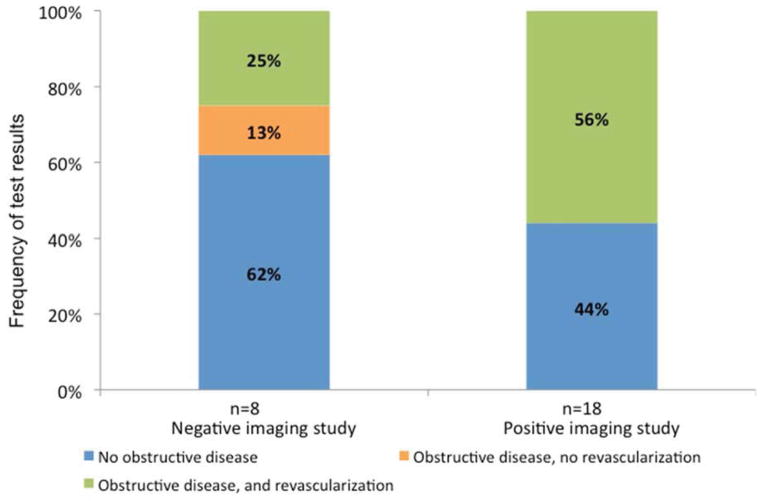
Methods: We followed consecutive individuals without known coronary artery disease referred for clinical ETT at a large medical center. We measured the frequency and results of downstream imaging tests and invasive angiography within 6 months of ETT and the combined endpoint of survival free from cardiovascular death, myocardial infarction, and coronary revascularization.
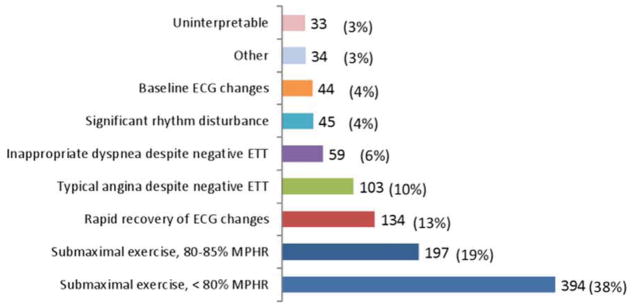
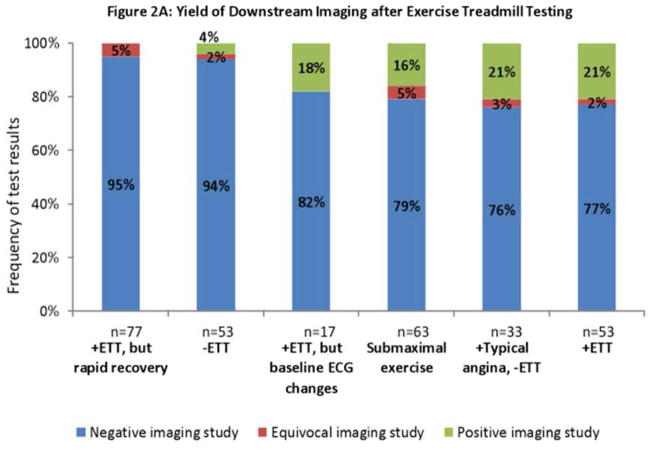
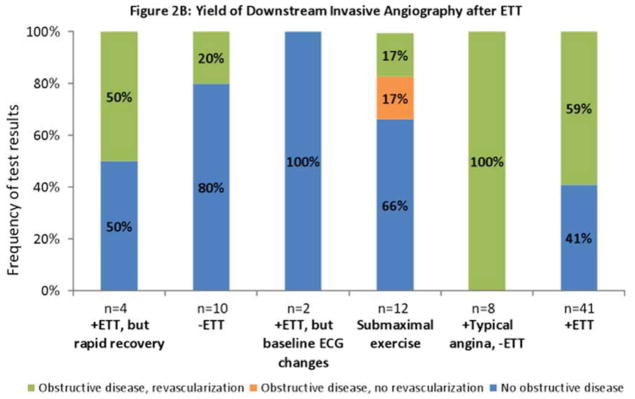
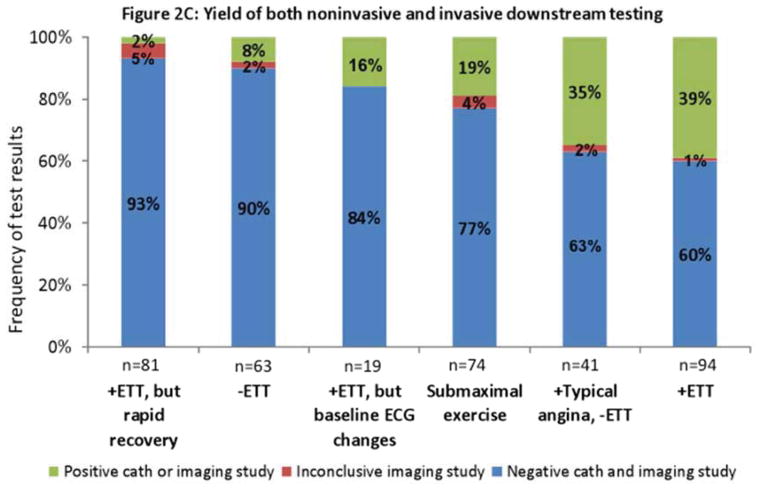
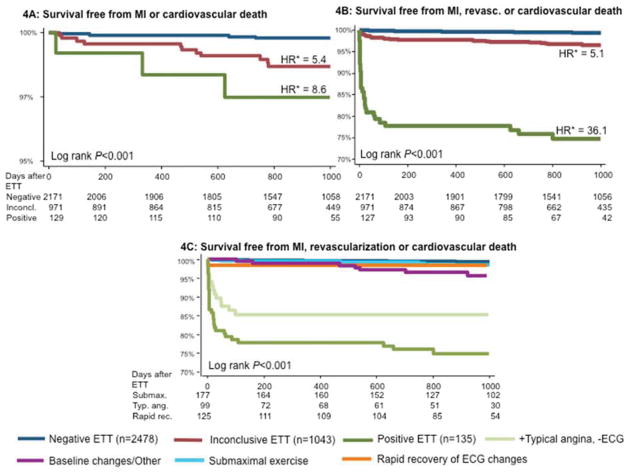
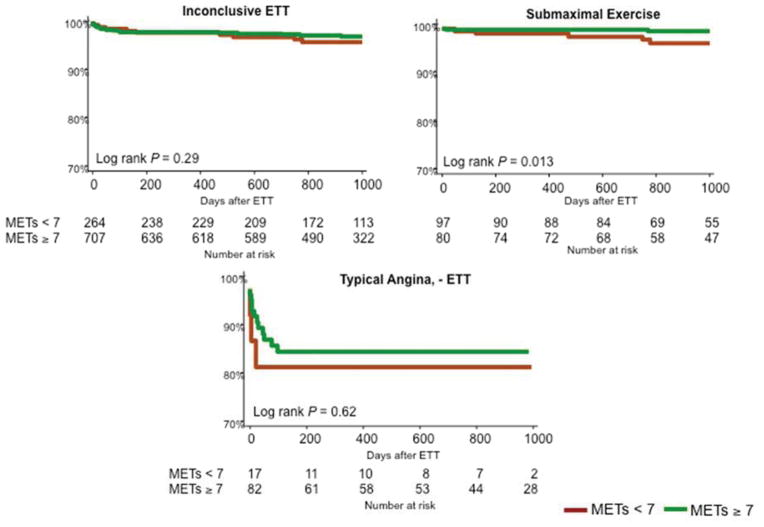
Results: Among 3,656 consecutive subjects who were followed for a mean of 2.5 ± 1.1 years, 332 (9.0%) underwent noninvasive imaging and 84 (2.3%) were referred directly to invasive angiography after ETT. The combined endpoint occurred in 76 (2.2%) patients. The annual incidence of the combined endpoint after negative, inconclusive, and positive ETT was 0.2%, 1.3%, and 12.4%, respectively (p < 0.001). Rapid recovery of electrocardiography (ECG) changes during ETT was associated with negative downstream test results and excellent prognosis, whereas typical angina despite negative ECG was associated with positive downstream tests and adverse prognosis (p < 0.001). Younger age, female sex, higher metabolic equivalents of task achieved, and rapid recovery of ECG changes were predictors of negative downstream tests.
Conclusions: Among patients referred for additional testing after ETT, the lowest yield was observed among individuals with rapid recovery of ECG changes or negative ETT, whereas the highest yield was observed among those with typical angina despite negative ECG or a positive ETT. These findings may be used to identify patients who are most and least likely to benefit from additional testing.
Keywords: downstream testing; exercise testing; imaging.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
No conflicts of interest or relationships with industry exist.
Figures
Comment in
-
Reframing the interpretation and application of exercise electrocardiography.J Am Coll Cardiol. 2014 Apr 8;63(13):1275-1277. doi: 10.1016/j.jacc.2013.12.026. Epub 2014 Feb 5. J Am Coll Cardiol. 2014. PMID: 24509274 No abstract available.
References
-
- Iglehart JK. The new era of medical imaging--progress and pitfalls. The New England journal of medicine. 2006;354:2822–8. - PubMed
-
- Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines) Circulation. 2002;106:1883–92. - PubMed
-
- Hendel RC, Berman DS, Di Carli MF, et al. ACCF/ASNC/ACR/AHA/ASE/SCCT/SCMR/SNM 2009 appropriate use criteria for cardiac radionuclide imaging: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the American Society of Nuclear Cardiology, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the Society of Cardiovascular Computed Tomography, the Society for Cardiovascular Magnetic Resonance, and the Society of Nuclear Medicine. Circulation. 2009;119:e561–87. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
