

Contemporary prevalence of pretreatment urinary, sexual, hormonal, and bowel dysfunction: Defining the population at risk for harms of prostate cancer treatment
- PMID: 24510400
- PMCID: PMC4930672
- DOI: 10.1002/cncr.28563
Contemporary prevalence of pretreatment urinary, sexual, hormonal, and bowel dysfunction: Defining the population at risk for harms of prostate cancer treatment
Abstract
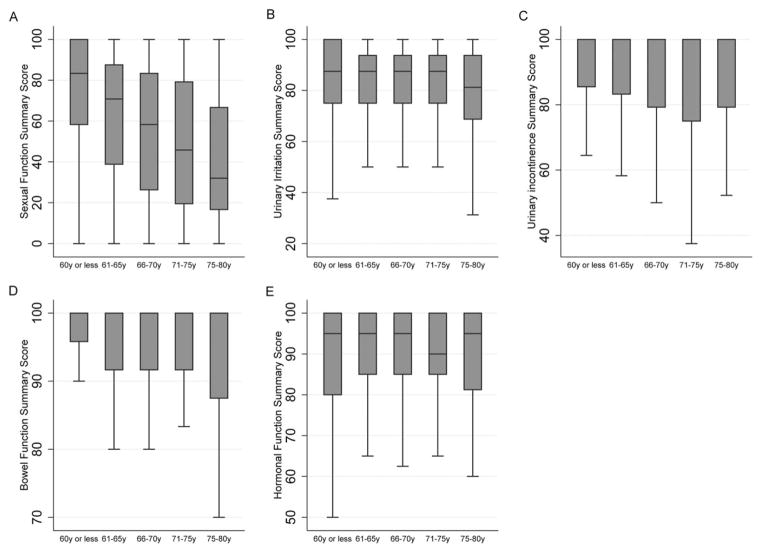
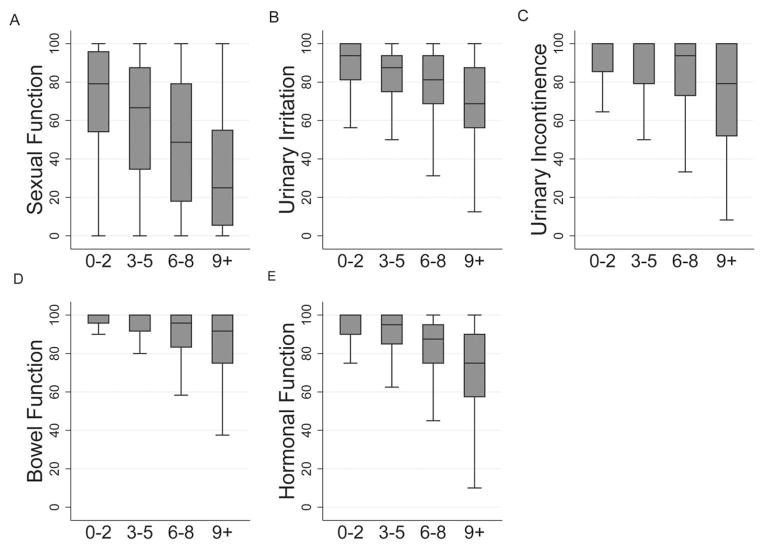
Background: The authors investigated the prevalence of pretreatment urinary, sexual, hormonal, and bowel dysfunction in a contemporary, population-based prostate cancer cohort. They also explored the associations between baseline function and age, comorbidity, and timing of baseline survey completion with respect to treatment.
Methods: The Comparative Effectiveness Analysis of Surgery and Radiation (CEASAR) study is a population-based, prospective cohort study that enrolled 3691 men with incident prostate cancer during 2011 and 2012. Pretreatment function was ascertained using the Expanded Prostate Cancer Index-26 (EPIC-26). Data were stratified by age, comorbidity, and timing of baseline survey completion with respect to treatment. Unadjusted and multivariable linear regression analyses were performed to evaluate the relations between exposures and pretreatment function.
Results: After applying exclusion criteria, the study cohort comprised 3072 men. A strikingly high proportion of men reported inability to obtain erections satisfactory for intercourse (45%) and some degree of urinary incontinence (17%) at baseline. Sexual function was particularly age-sensitive, with patients aged ≤60 years reporting summary scores in excess of 30 points higher than patients aged ≥75 years (P < .001). Compared with the healthiest men, highly comorbid patients reported less favorable function in each domain, including urinary incontinence (summary score, 89.5 vs 74.1; P < .001) and sexual function (summary score, 70.8 vs 32.9; P < .001). Although statistically significant differences in summary scores were identified between patients who completed the baseline questionnaire before treatment (52%) versus after treatment (48%), the absolute differences were small (range, 1-3 points).
Conclusions: Patients with newly diagnosed prostate cancer exhibit a wide distribution of pretreatment function. The current data may be used to redefine the population "at risk" for treatment-related harms.
Keywords: bowel function; prostate cancer; quality of life; sexual function; urinary function.
© 2014 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES
Dr. Resnick reports personal fees from Denreon and Photocure. Dr. Barocas reports personal fees from Janssen, GE Healthcare, and Dendreon. Dr. Morgans reports personal fees from Myriad. Dr. Cooperberg reports personal fees from Amgen, Dendreon, Genomic Health, Myriad, Genomedx, Abbott Laboratories, Astellas, and Janssen.
Figures
Similar articles
-
The Evolution of Self-Reported Urinary and Sexual Dysfunction over the Last Two Decades: Implications for Comparative Effectiveness Research.Eur Urol. 2015 Jun;67(6):1019-1025. doi: 10.1016/j.eururo.2014.08.035. Epub 2014 Aug 28. Eur Urol. 2015. PMID: 25174325 Free PMC article.
-
Development and Internal Validation of a Web-based Tool to Predict Sexual, Urinary, and Bowel Function Longitudinally After Radiation Therapy, Surgery, or Observation.Eur Urol. 2020 Aug;78(2):248-255. doi: 10.1016/j.eururo.2020.02.007. Epub 2020 Feb 22. Eur Urol. 2020. PMID: 32098731 Free PMC article.
-
Regional Variations in Quality of Survival Among Men with Prostate Cancer Across the United Kingdom.Eur Urol. 2019 Aug;76(2):228-237. doi: 10.1016/j.eururo.2019.04.018. Epub 2019 May 4. Eur Urol. 2019. PMID: 31060822
-
Quality of life study in prostate cancer patients treated with three-dimensional conformal radiation therapy: comparing late bowel and bladder quality of life symptoms to that of the normal population.Int J Radiat Oncol Biol Phys. 2001 Jan 1;49(1):51-9. doi: 10.1016/s0360-3016(00)01365-1. Int J Radiat Oncol Biol Phys. 2001. PMID: 11163497 Review.
-
How to present quality of life outcomes after focal therapy: using validated instruments and novel statistical methods.Curr Opin Urol. 2022 May 1;32(3):254-259. doi: 10.1097/MOU.0000000000000974. Epub 2022 Feb 23. Curr Opin Urol. 2022. PMID: 35199651 Review.
Cited by
-
Determinants of self-reported functional status (EPIC-26) in prostate cancer patients prior to treatment.World J Urol. 2021 Jan;39(1):27-36. doi: 10.1007/s00345-020-03097-z. Epub 2020 Feb 10. World J Urol. 2021. PMID: 32040715 Free PMC article.
-
Changes in Nocturia and Lower Urinary Tract Symptoms after Radical Prostatectomy.World J Mens Health. 2015 Dec;33(3):194-201. doi: 10.5534/wjmh.2015.33.3.194. Epub 2015 Dec 23. World J Mens Health. 2015. PMID: 26770940 Free PMC article.
-
Treatment Decision Regret Among Long-Term Survivors of Localized Prostate Cancer: Results From the Prostate Cancer Outcomes Study.J Clin Oncol. 2017 Jul 10;35(20):2306-2314. doi: 10.1200/JCO.2016.70.6317. Epub 2017 May 11. J Clin Oncol. 2017. PMID: 28493812 Free PMC article.
-
Impact of Age on Patient-Reported Outcomes Following Stereotactic Body Radiation Therapy for Prostate Cancer.Cureus. 2021 Mar 9;13(3):e13780. doi: 10.7759/cureus.13780. Cureus. 2021. PMID: 33842156 Free PMC article.
-
Radiotherapy after radical prostatectomy: Effect of timing of postprostatectomy radiation on functional outcomes.Urol Oncol. 2020 Dec;38(12):930.e23-930.e32. doi: 10.1016/j.urolonc.2020.06.022. Epub 2020 Jul 29. Urol Oncol. 2020. PMID: 32736934 Free PMC article.
References
-
- Zeliadt SB, Moinpour CM, Blough DK, et al. Preliminary treatment considerations among men with newly diagnosed prostate cancer [serial online] Am J Manag Care. 2010;16:e121–e130. - PubMed
-
- Zeliadt SB, Ramsey SD, Penson DF, et al. Why do men choose 1 treatment over another? A review of patient decision making for localized prostate cancer. Cancer. 2006;106:1865–1874. - PubMed
-
- Sanda MG, Dunn RL, Michalski J, et al. Quality of life and satisfaction with outcome among prostate-cancer survivors. N Engl J Med. 2008;358:1250–1261. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
