

Use of ultrasonography in developmental dysplasia of the hip
- PMID: 24510434
- PMCID: PMC3965765
- DOI: 10.1007/s11832-014-0561-8
Use of ultrasonography in developmental dysplasia of the hip
Abstract
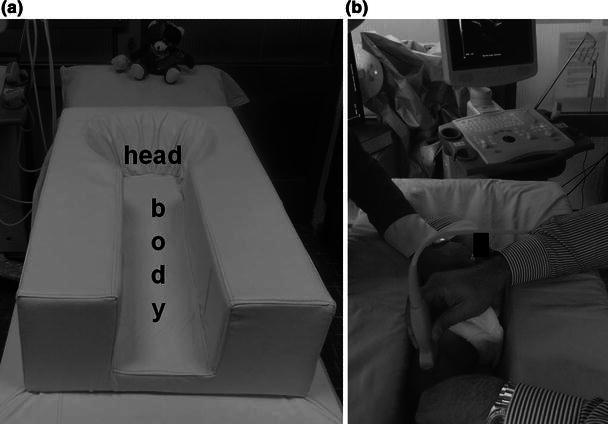
Purpose: Ultrasonography has been used as a diagnostic tool in developmental dysplasia of the hip (DDH) during early infancy since the early 1980s. The aim of this review article is to summarise the technique, benefits and shortcomings of four infantile hip ultrasonography methods, focusing mainly on the Graf method, and to assess the effectiveness of ultrasonographic newborn hip screening programmes.
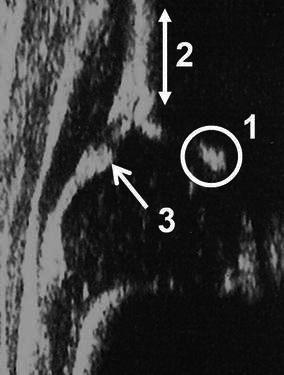
Methods: Several infantile hip ultrasonography methods have been defined to assess the relationship between the femoral head and acetabulum. The Graf, Harcke, Terjesen and Suzuki methods are the universally known ones. The Graf method is composed of a quantitative classification system, while the Harcke and Suzuki methods have qualitative definitions and the Terjesen method contains both quantitative and qualitative descriptions.
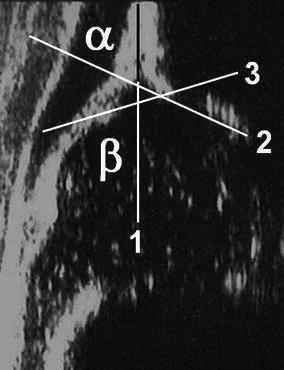
Results: Although the results of several studies assessing the sensitivity and consistency of the ultrasonography methods have still not proven a clear dominance of one of these techniques, the primary advantage of the Graf method is that it has a standardised examination technique, as well as a very well defined numeric hip typing system. The importance of newborn hip screening has been universally accepted, but there is still no strong evidence regarding the superiority of either universal (screening of all newborns) or selective (screening of high-risk newborns) ultrasonographic newborn hip screening programmes.
Conclusions: An effective ultrasonographic method should include simple, precise, quantitative and consistent definitions for a proper examination and diagnosis. Both universal and selective ultrasonographic newborn hip screening programmes have significantly decreased the rate of late detected DDH and lessened the need for surgical treatment.
Figures



References
-
- Wientroub S, Grill F. Ultrasonography in developmental dysplasia of the hip. J Bone Joint Surg Am. 2000;82-A:1004–1018. - PubMed
-
- Graf R. Hip sonography. Diagnosis and management of infant hip dysplasia. 2. Berlin: Springer; 2006.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
