

Comprehensive immunophenotyping of cerebrospinal fluid cells in patients with neuroimmunological diseases
- PMID: 24510966
- PMCID: PMC4045479
- DOI: 10.4049/jimmunol.1302884
Comprehensive immunophenotyping of cerebrospinal fluid cells in patients with neuroimmunological diseases
Abstract
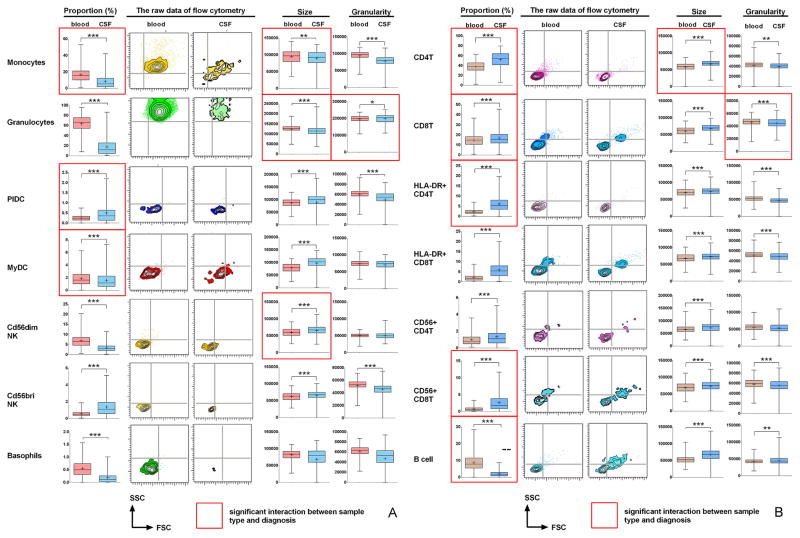
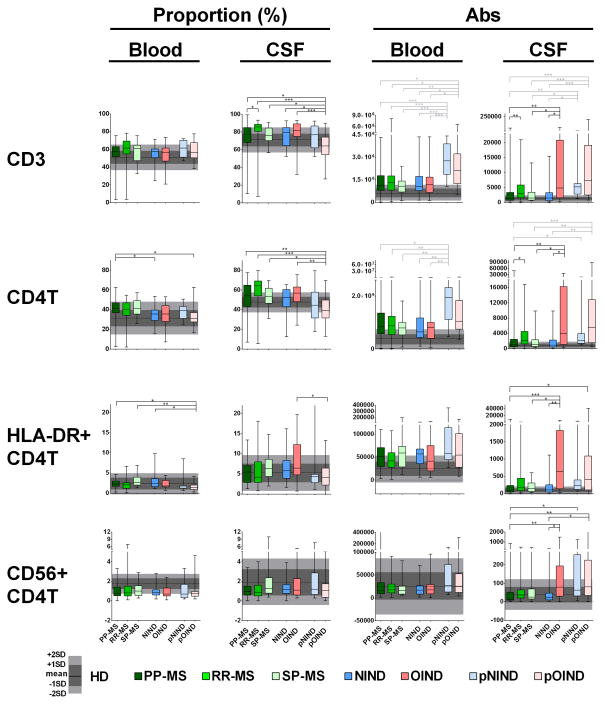
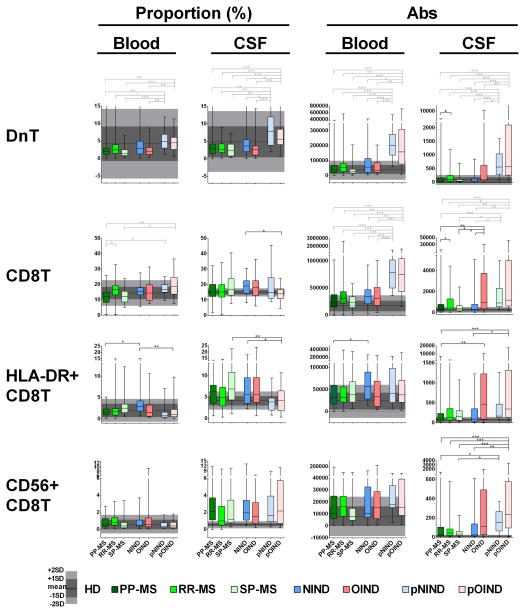
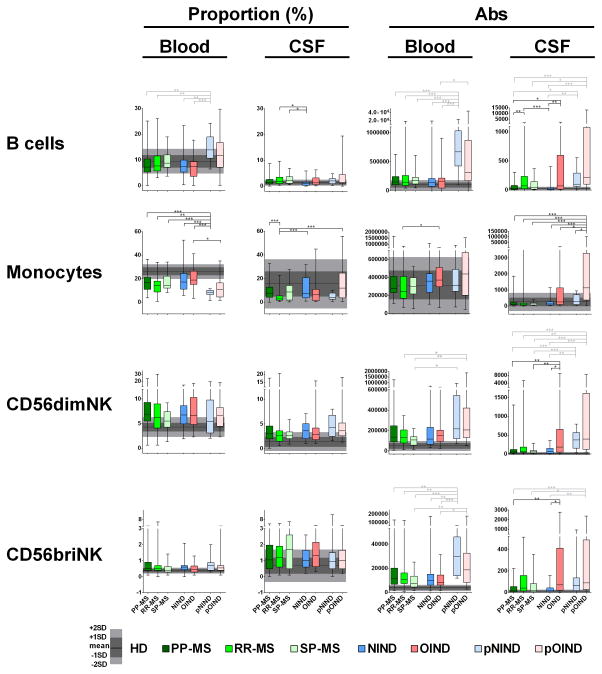
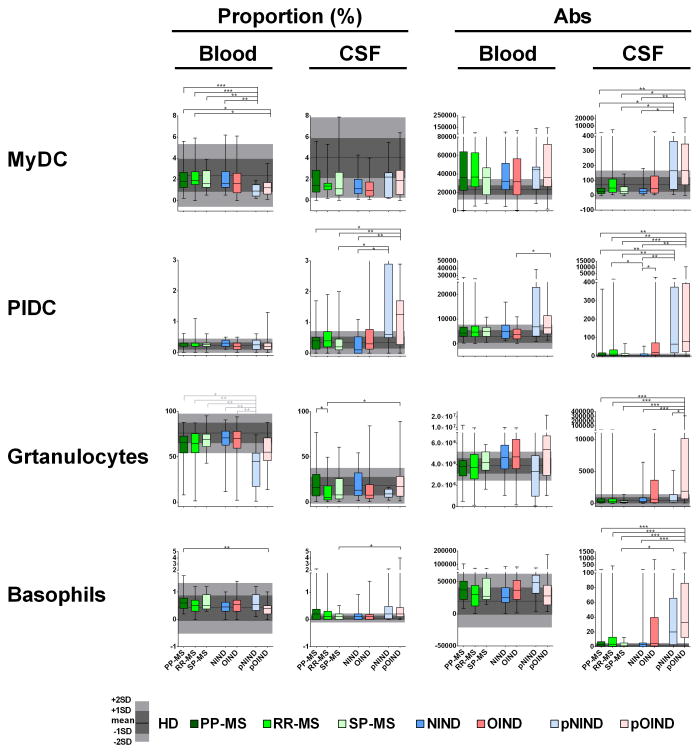
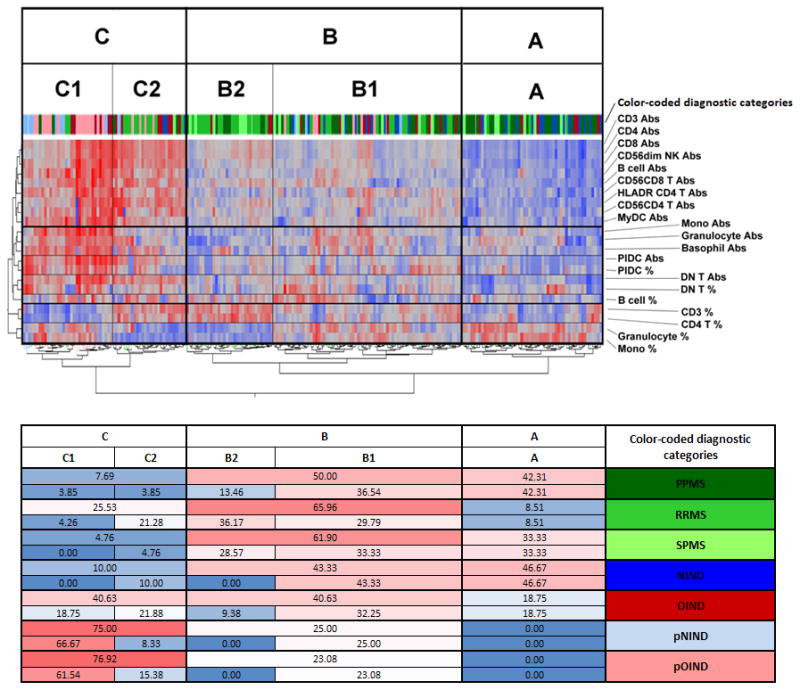
We performed unbiased, comprehensive immunophenotyping of cerebrospinal fluid (CSF) and blood leukocytes in 221 subjects referred for the diagnostic work-up of neuroimmunological disorders to obtain insight about disease-specific phenotypes of intrathecal immune responses. Quantification of 14 different immune cell subsets, coupled with the assessment of their activation status, revealed physiological differences between intrathecal and systemic immunity, irrespective of final diagnosis. Our data are consistent with a model where the CNS shapes intrathecal immune responses to provide effective protection against persistent viral infections, especially by memory T cells, plasmacytoid dendritic cells, and CD56(bright) NK cells. Our data also argue that CSF immune cells do not simply reflect cells recruited from the periphery. Instead, they represent a mixture of cells that are recruited from the blood, have been activated intrathecally and leave the CNS after performing effector functions. Diagnosis-specific differences provide mechanistic insight into the disease process in the defined subtypes of multiple sclerosis (MS), neonatal onset multisystem inflammatory disease, and Aicardi-Goutières syndrome. This analysis also determined that secondary-progressive MS patients are immunologically closer to relapsing-remitting patients as compared with patients with primary-progressive MS. Because CSF immunophenotyping captures the biology of the intrathecal inflammatory processes, it has the potential to guide optimal selection of immunomodulatory therapies in individual patients and monitor their efficacy. Our study adds to the increasing number of publications that demonstrate poor correlation between systemic and intrathecal inflammatory biomarkers in patients with neuroimmunological diseases and stresses the importance of studying immune responses directly in the intrathecal compartment.
Figures
References
-
- Miller DH, Leary SM. Primary-progressive multiple sclerosis. Lancet neurology. 2007;6:903–912. - PubMed
-
- Sastre-Garriga J, Ingle GT, Chard DT, Cercignani M, Ramio-Torrenta L, Miller DH, Thompson AJ. Grey and white matter volume changes in early primary progressive multiple sclerosis: a longitudinal study. Brain. 2005;128:1454–1460. - PubMed
-
- Lucchinetti C, Bruck W. The pathology of primary progressive multiple sclerosis. Mult Scler. 2004;10(Suppl 1):S23–30. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
