

Kidney transplantation with early corticosteroid withdrawal: paradoxical effects at the central and peripheral skeleton
- PMID: 24511131
- PMCID: PMC4033378
- DOI: 10.1681/ASN.2013080851
Kidney transplantation with early corticosteroid withdrawal: paradoxical effects at the central and peripheral skeleton
Abstract
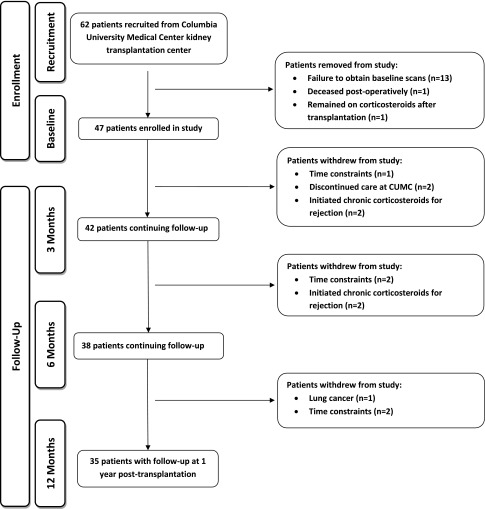
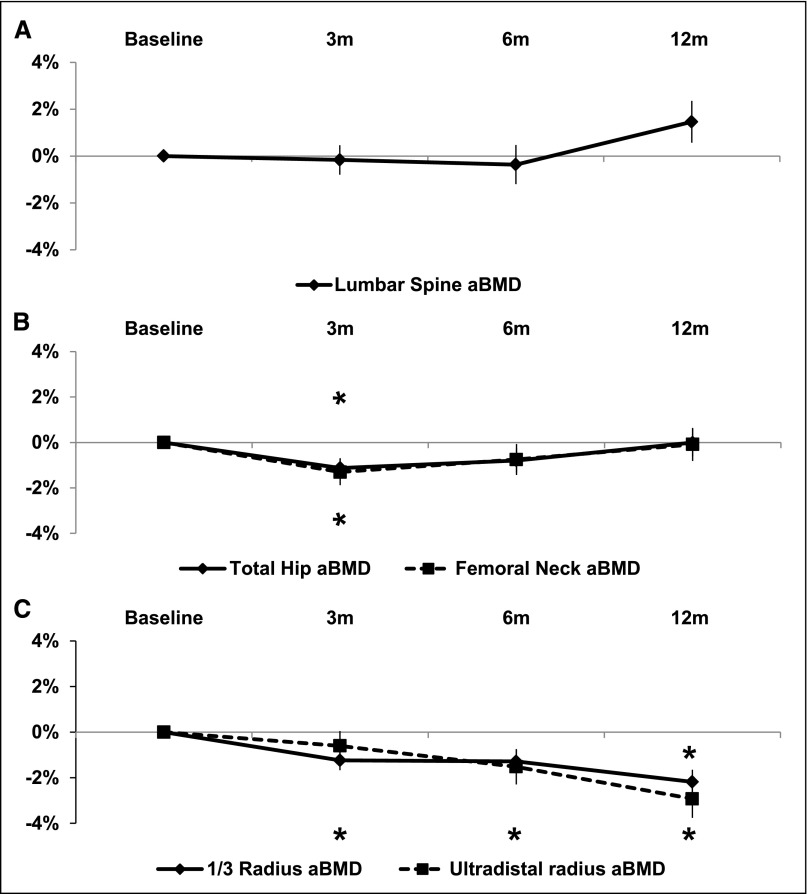
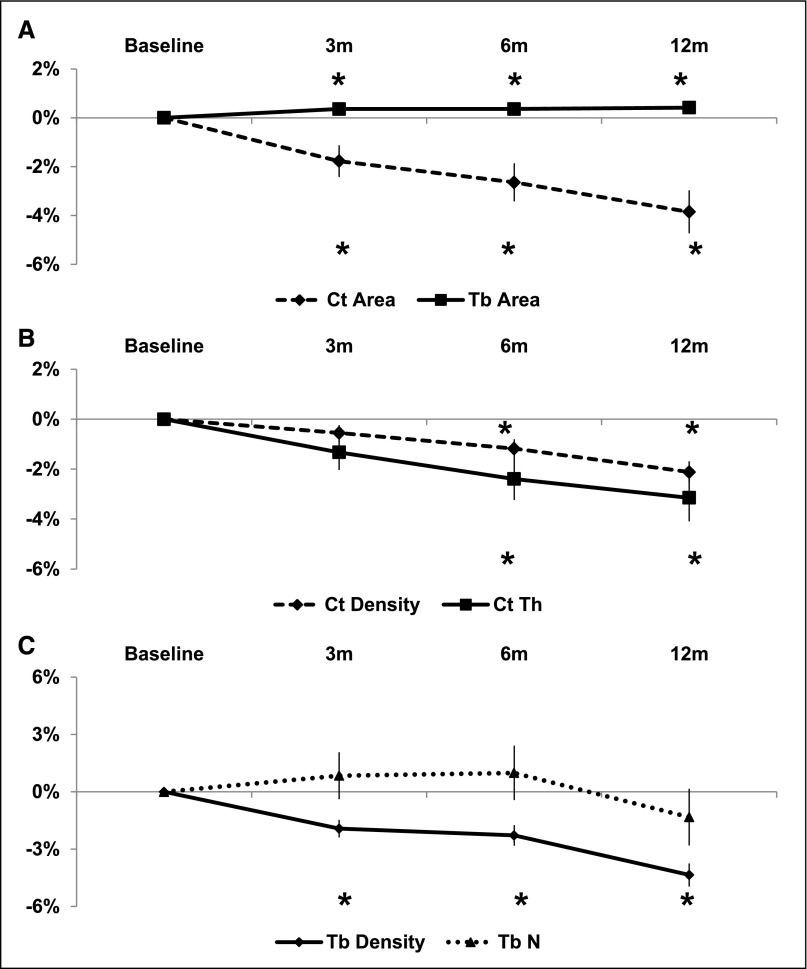
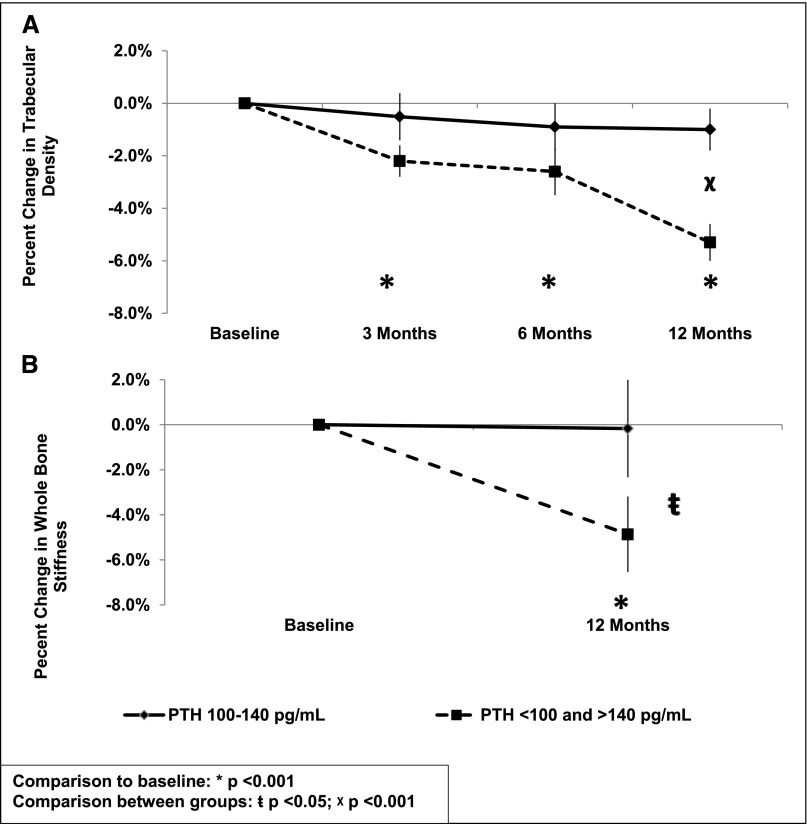
The use of early corticosteroid withdrawal (ECSW) protocols after kidney transplantation has become common, but the effects on fracture risk and bone quality are unclear. We enrolled 47 first-time adult transplant recipients managed with ECSW into a 1-year study to evaluate changes in bone mass, microarchitecture, biomechanical competence, and remodeling with dual energy x-ray absorptiometry (DXA), high-resolution peripheral quantitative computed tomography (HRpQCT), parathyroid hormone (PTH) levels, and bone turnover markers obtained at baseline and 3, 6, and 12 months post-transplantation. Compared with baseline, 12-month areal bone mineral density by DXA did not change significantly at the spine and hip, but it declined significantly at the 1/3 and ultradistal radii (2.2% and 2.9%, respectively; both P<0.001). HRpQCT of the distal radius revealed declines in cortical area, density, and thickness (3.9%, 2.1%, and 3.1%, respectively; all P<0.001), trabecular density (4.4%; P<0.001), and stiffness and failure load (3.1% and 3.5%, respectively; both P<0.05). Findings were similar at the tibia. Increasing severity of hyperparathyroidism was associated with increased cortical losses. However, loss of trabecular bone and bone strength were most severe at the lowest and highest PTH levels. In summary, ECSW was associated with preservation of bone mineral density at the central skeleton; however, it was also associated with progressive declines in cortical and trabecular bone density at the peripheral skeleton. Cortical decreases related directly to PTH levels, whereas the relationship between PTH and trabecular bone decreases was bimodal. Studies are needed to determine whether pharmacologic agents that suppress PTH will prevent cortical and trabecular losses and post-transplant fractures.
Copyright © 2014 by the American Society of Nephrology.
Figures

References
-
- Nikkel LE, Hollenbeak CS, Fox EJ, Uemura T, Ghahramani N: Risk of fractures after renal transplantation in the United States. Transplantation 87: 1846–1851, 2009 - PubMed
-
- Ball AM, Gillen DL, Sherrard D, Weiss NS, Emerson SS, Seliger SL, Kestenbaum BR, Stehman-Breen C: Risk of hip fracture among dialysis and renal transplant recipients. JAMA 288: 3014–3018, 2002 - PubMed
-
- Abbott KC, Oglesby RJ, Hypolite IO, Kirk AD, Ko CW, Welch PG, Agodoa LY, Duncan WE: Hospitalizations for fractures after renal transplantation in the United States. Ann Epidemiol 11: 450–457, 2001 - PubMed
-
- Vautour LM, Melton LJ, 3rd, Clarke BL, Achenbach SJ, Oberg AL, McCarthy JT: Long-term fracture risk following renal transplantation: A population-based study. Osteoporos Int 15: 160–167, 2004 - PubMed
-
- Julian BA, Laskow DA, Dubovsky J, Dubovsky EV, Curtis JJ, Quarles LD: Rapid loss of vertebral mineral density after renal transplantation. N Engl J Med 325: 544–550, 1991 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
