

Shear stress, energy losses, and costs: a resolved dilemma of pulsatile cardiac assist devices
- PMID: 24511541
- PMCID: PMC3913384
- DOI: 10.1155/2014/651769
Shear stress, energy losses, and costs: a resolved dilemma of pulsatile cardiac assist devices
Abstract
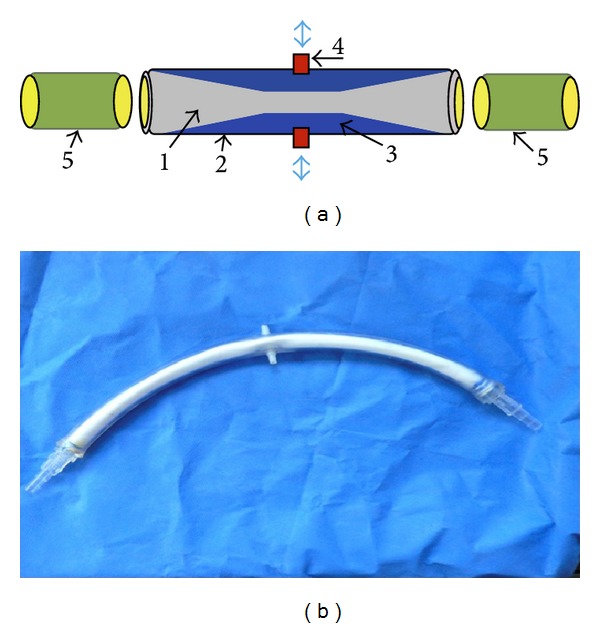
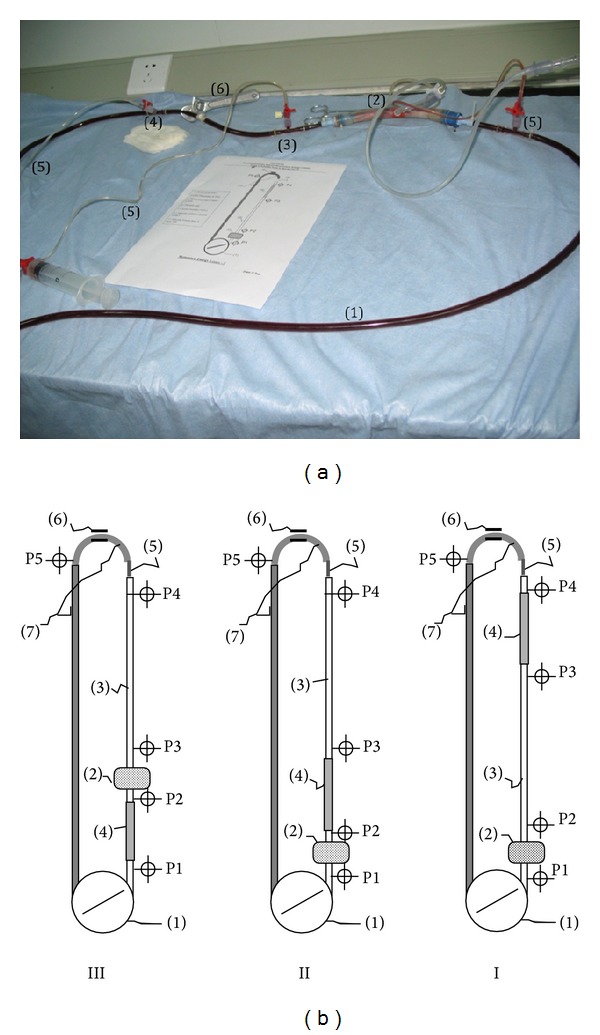
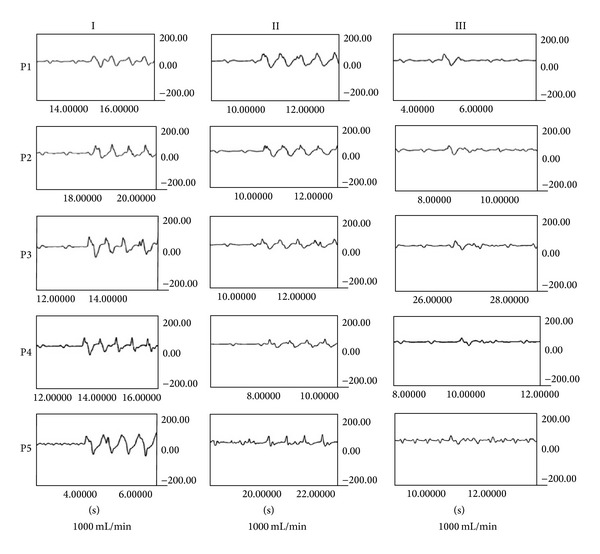
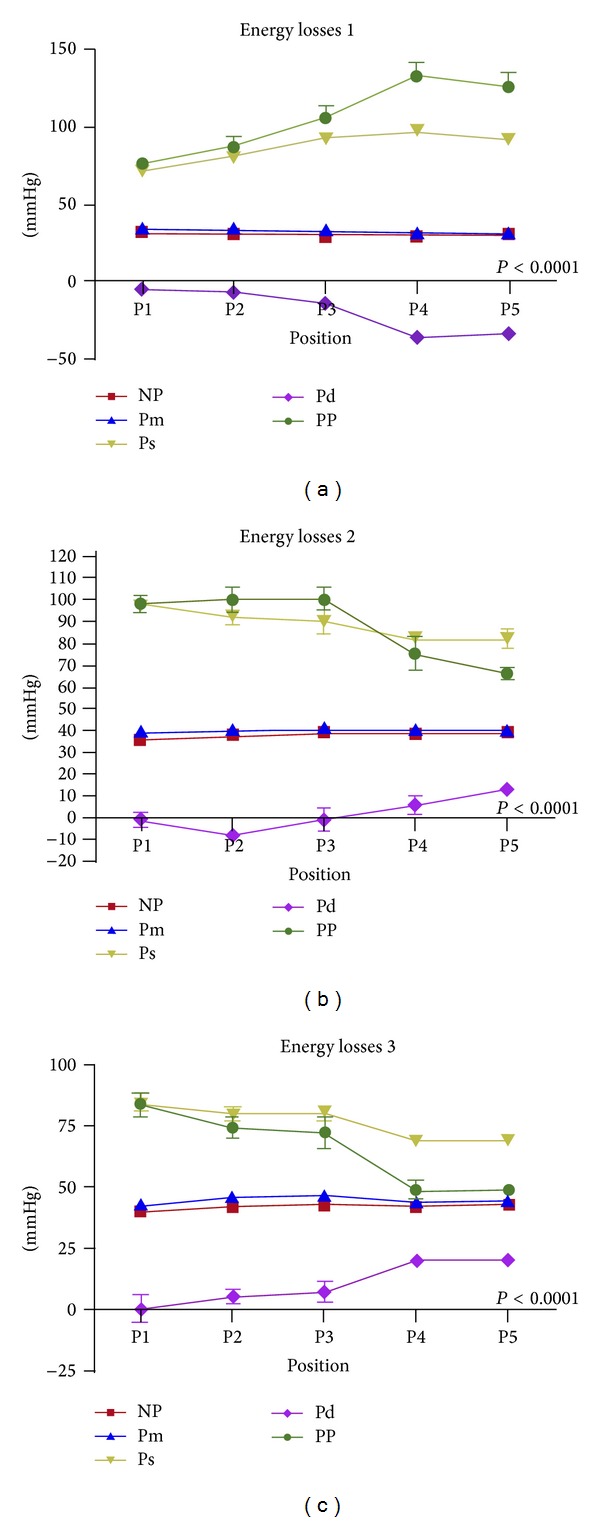
Cardiac assist devices (CAD) cause endothelial dysfunction with considerable morbidity. Employment of pulsatile CAD remains controversial due to inadequate perfusion curves and costs. Alternatively, we are proposing a new concept of pulsatile CAD based on a fundamental revision of the entire circulatory system in correspondence with the physiopathology and law of physics. It concerns a double lumen disposable tube device that could be adapted to conventional cardiopulmonary bypass (CPB) and/or CAD, for inducing a homogenous, downstream pulsatile perfusion mode with lower energy losses. In this study, the device's prototypes were tested in a simulated conventional pediatric CPB circuit for energy losses and as a left ventricular assist device (LVAD) in ischemic piglets model for endothelial shear stress (ESS) evaluations. In conclusion and according to the study results the pulsatile tube was successfully capable of transforming a conventional CPB and/or CAD steady flow into a pulsatile perfusion mode, with nearly physiologic pulse pressure and lower energy losses. This represents a cost-effective promising method with low mortality and morbidity, especially in fragile cardiac patients.
Figures
References
-
- Diehl P, Aleker M, Helbing T, et al. Enhanced microparticles in ventricular assist device patients predict platelet, leukocyte and endothelial cell activation. Interactive CardioVasc Thoracic Surgery. 2010;11:133–137. - PubMed
-
- Pieske B. Reverse remodeling in heart failure—fact or fiction? European Heart Journal, Supplement. 2004;6:D66–D78.
-
- Habazettl H, Kukucka M, Weng YG, et al. Arteriolar blood flow pulsatility in a patient before and after implantation of an axial flow pump. Annals of Thoracic Surgery. 2006;81(3):1109–1111. - PubMed
-
- McHugh J, Cheek DJ. Nitric oxide and regulation of vascular tone: pharmacological and physiological considerations. The American Journal of Critical Care. 1998;7(2):131–140. - PubMed
-
- Thorin E, Nguyen T-D, Bouthillier A. Control of vascular tone by endogenous endothelin-1 in human pial arteries. Stroke. 1998;29(1):175–180. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
