

Pathogenesis and prevention of rheumatic disease: focus on preclinical RA and SLE
- PMID: 24514912
- PMCID: PMC4090326
- DOI: 10.1038/nrrheum.2014.6
Pathogenesis and prevention of rheumatic disease: focus on preclinical RA and SLE
Abstract
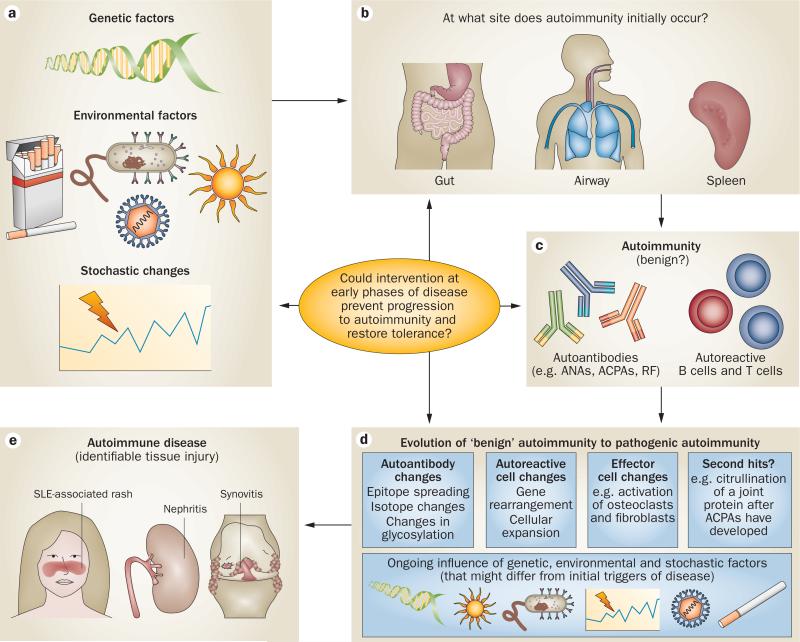
Established and emerging data demonstrate that a 'preclinical' period of disease precedes the onset of clinical rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE), as well as other autoimmune rheumatic diseases (ARDs).This preclinical stage of development of disease is characterized by abnormalities in disease-related biomarkers before the onset of the clinically apparent signs and symptoms. Numerous genetic and environmental risk factors for ARDs have also been identified, and many of these factors are likely to act before the clinical appearance of tissue injury to initiate and/or propagate autoimmunity and autoimmune disease. Thus, biomarkers representative of these autoimmune processes could potentially be used in conjunction with other clinical parameters during the preclinical period of ARDs to predict the future development of clinically apparent disease. This Review focuses on the preclinical stages of RA and SLE, as our current understanding of these diseases can be used to present an overall model of the development of ARDs that might ultimately be used to develop screening programmes and preventive strategies. Important considerations for the future development of such approaches, in particular, the issues that require additional research and how they might be addressed, are also discussed.
Figures

References
-
- Helmick CG, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part I. Arthritis Rheum. 2007;58:15–25. - PubMed
-
- Jacobson DL, Gange SJ, Rose NR, Graham NM. Epidemiology and estimated population burden of selected autoimmune diseases in the United States. Clin. Immunol. Immunopathol. 1997;84:223–243. - PubMed
-
- Birnbaum H, et al. Societal cost of rheumatoid arthritis patients in the US. Curr. Med. Res. Opin. 2010;26:77–90. - PubMed
-
- Proceedings. Isr. J. Med. Sci. Vol. 26. Tel-Hashomer, Israel: Jan 25, 1990. Fourth autoimmunity meeting—Noel Rose day. pp. 661–718. [No authors listed] 1990. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
