

Effect of clinical pharmacist intervention on medication discrepancies following hospital discharge
- PMID: 24515550
- PMCID: PMC4026363
- DOI: 10.1007/s11096-014-9917-x
Effect of clinical pharmacist intervention on medication discrepancies following hospital discharge
Abstract
Background: Medication discrepancies may occur at transitions in care and negatively impact patient outcomes.
Objective: To determine if involving clinical pharmacists in hospital care, medication reconciliation and discharge medication plan communication can reduce medication discrepancies with a prospective, randomized, blinded, controlled trial.
Setting: A large, tertiary care, academic medical center.
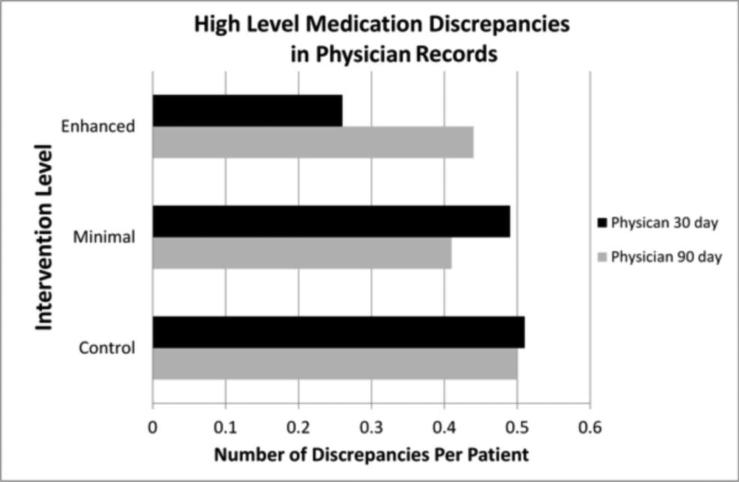
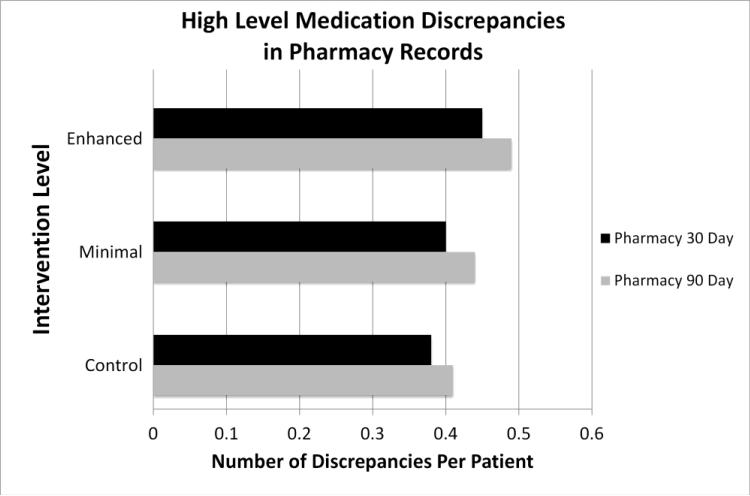
Method: The intervention consisted of clinical pharmacist medication reconciliation, patient education and improved communication of the discharge medication plan, as devised by the hospital physician and care team, to primary care physicians and community pharmacists. Medication discrepancies were identified by blinded research pharmacists who reviewed primary care physician and pharmacy records at discharge through 90 days post-discharge to create 30- and 90-day medication lists.
Main outcome measure: Rate of medication discrepancies compared across groups.
Results: A total of 592 subjects from internal medicine, family medicine, cardiology and orthopedic services were evaluated for this study. Clinically important medication discrepancies in the primary care physician record were different between groups 30 days after hospital discharge following a clinical pharmacist's intervention. The mean number of medication discrepancies per patient for the enhanced group being nearly half the number in the control group. However, this effect did not persist to 90 days post-discharge and did not extend to community pharmacy records.
Conclusion: The present study demonstrates the involvement of pharmacists in hospital care, medication reconciliation and discharge medication plan communication may affect the quality of the outpatient medical record.
Figures
References
-
- Rozich JD, Resar RK. Medication safety: one organization's approach to the challenge. J Clin Outcomes Manag. 2001;8(10):27–34.
-
- Rozich JD, Howard RJ, Justeson JM, Macken PD, Lindsay ME, Resar RK. Standardization as a mechanism to improve safety in health care. Jt Comm J Qual Saf. 2004;30(1):5–14. - PubMed
-
- Green CF, Burgul K, Armstrong DJ. A study of the use of medicine lists in medicines reconciliation: please remember this, a list is just a list. Int J Pharm Pract. 2010;18(2):116–21. - PubMed
-
- Coleman EA, Smith JD, Raha D, Min SJ. Posthospital medication discrepancies: prevalence and contributing factors. Arch Intern Med. 2005;165(16):1842–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
