

Extent of resection of glioblastoma revisited: personalized survival modeling facilitates more accurate survival prediction and supports a maximum-safe-resection approach to surgery
- PMID: 24516010
- PMCID: PMC4876349
- DOI: 10.1200/JCO.2013.51.8886
Extent of resection of glioblastoma revisited: personalized survival modeling facilitates more accurate survival prediction and supports a maximum-safe-resection approach to surgery
Abstract
Purpose: Approximately 12,000 glioblastomas are diagnosed annually in the United States. The median survival rate for this disease is 12 months, but individual survival rates can vary with patient-specific factors, including extent of surgical resection (EOR). The goal of our investigation is to develop a reliable strategy for personalized survival prediction and for quantifying the relationship between survival, EOR, and adjuvant chemoradiotherapy.
Patients and methods: We used accelerated failure time (AFT) modeling using data from 721 newly diagnosed patients with glioblastoma (from 1993 to 2010) to model the factors affecting individualized survival after surgical resection, and we used the model to construct probabilistic, patient-specific tools for survival prediction. We validated this model with independent data from 109 patients from a second institution.
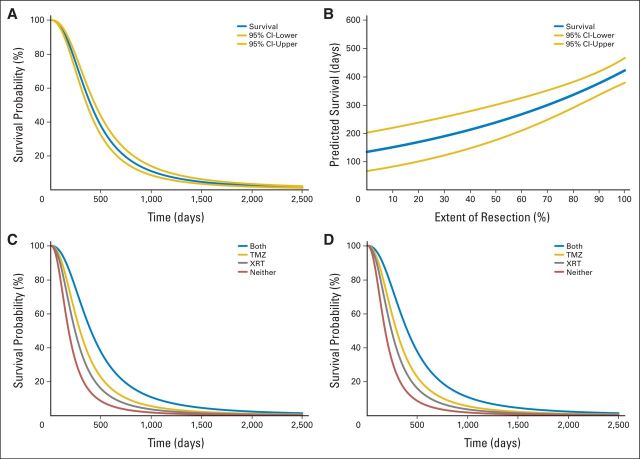
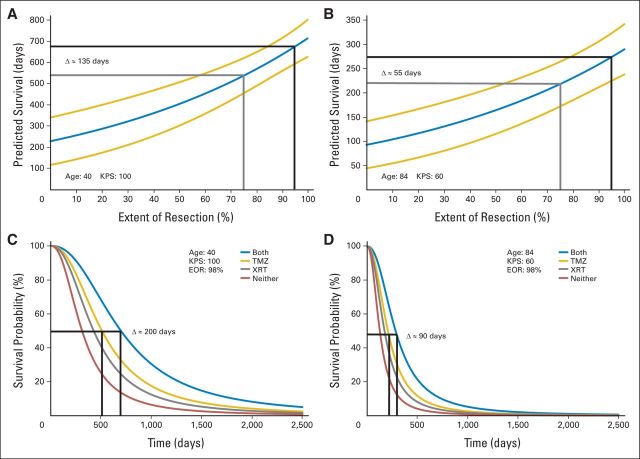
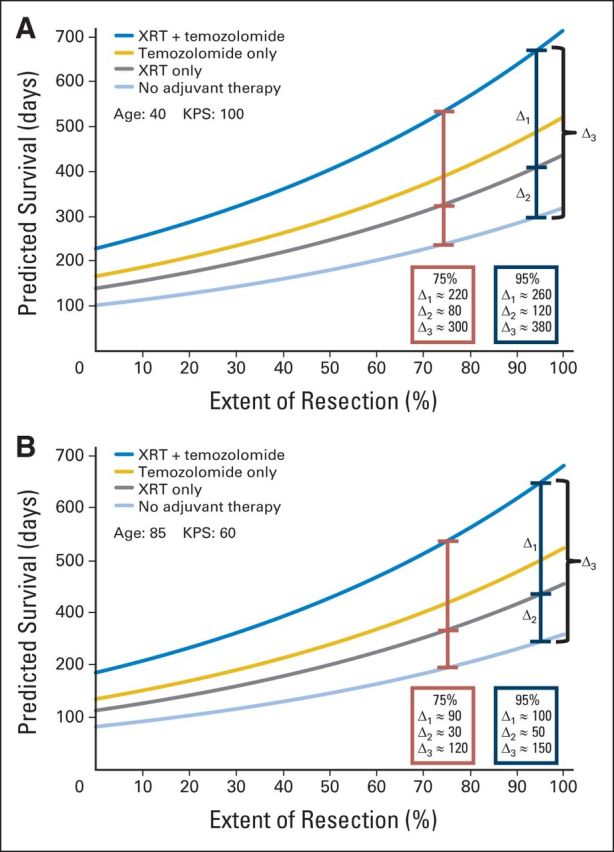
Results: AFT modeling using age, Karnofsky performance score, EOR, and adjuvant chemoradiotherapy produced a continuous, nonlinear, multivariable survival model for glioblastoma. The median personalized predictive error was 4.37 months, representing a more than 20% improvement over current methods. Subsequent model-based calculations yield patient-specific predictions of the incremental effects of EOR and adjuvant therapy on survival.
Conclusion: Nonlinear, multivariable AFT modeling outperforms current methods for estimating individual survival after glioblastoma resection. The model produces personalized survival curves and quantifies the relationship between variables modulating patient-specific survival. This approach provides comprehensive, personalized, probabilistic, and clinically relevant information regarding the anticipated course of disease, the overall prognosis, and the patient-specific influence of EOR and adjuvant chemoradiotherapy. The continuous, nonlinear relationship identified between expected median survival and EOR argues against a surgical management strategy based on rigid EOR thresholds and instead provides the first explicit evidence supporting a maximum safe resection approach to glioblastoma surgery.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Maximum safe resection of glioblastoma multiforme.J Clin Oncol. 2014 Mar 10;32(8):727-8. doi: 10.1200/JCO.2013.53.2788. Epub 2014 Feb 10. J Clin Oncol. 2014. PMID: 24516027 No abstract available.
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987–996. - PubMed
-
- Mirimanoff RO, Gorlia T, Mason W, et al. Radiotherapy and temozolomide for newly diagnosed glioblastoma: Recursive partitioning analysis of the EORTC 26981/22981-NCIC CE3 phase III randomized trial. J Clin Oncol. 2006;24:2563–2569. - PubMed
-
- Sanai N, Polley MY, McDermott MW, et al. An extent of resection threshold for newly diagnosed glioblastomas. J Neurosurg. 2011;115:3–8. - PubMed
-
- Sanai N, Berger MS. Extent of resection influences outcomes for patients with gliomas. Rev Neurol (Paris) 2011;167:648–654. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
