

A systematic review of surgical ablation versus catheter ablation for atrial fibrillation
- PMID: 24516794
- PMCID: PMC3904326
- DOI: 10.3978/j.issn.2225-319X.2014.01.03
A systematic review of surgical ablation versus catheter ablation for atrial fibrillation
Abstract
Background: Atrial fibrillation (AF) is an increasingly prevalent condition in the ageing population, with significantly associated morbidity and mortality. Surgical and catheter ablative strategies both aim to reduce mortality and morbidity through freedom from AF. This review consolidates all currently available comparative data to evaluate these two interventions.
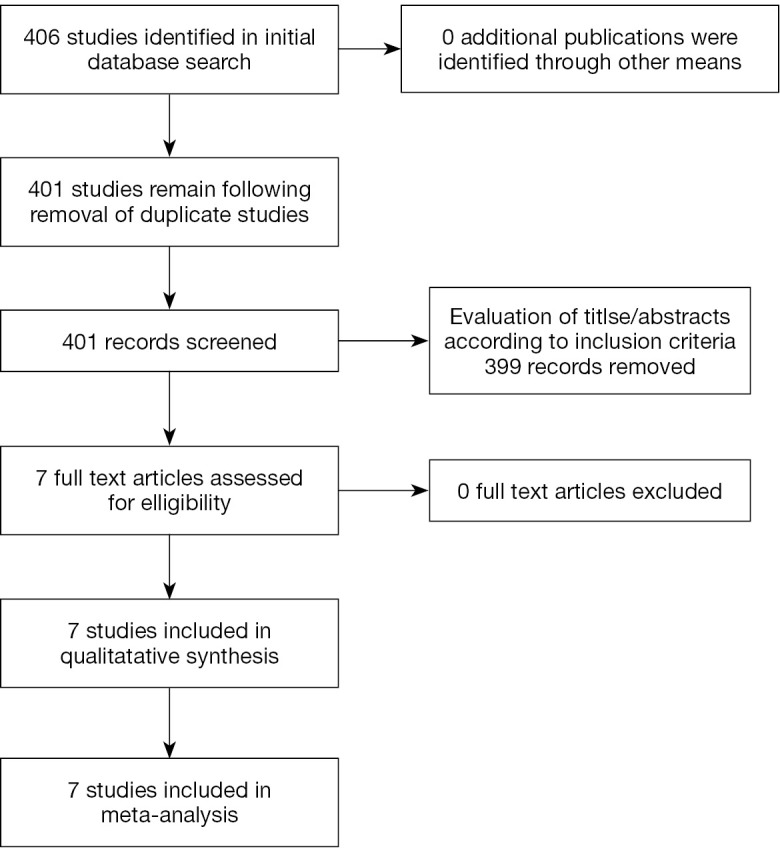
Methods: A systematic search was conducted across MEDLINE, PubMed, Embase, Cochrane Central Register of Controlled Trials and the Cochrane Database of Systematic Reviews from January 2000 until August 2013. All studies were critically appraised and only those directly comparing surgical and catheter ablation were included.
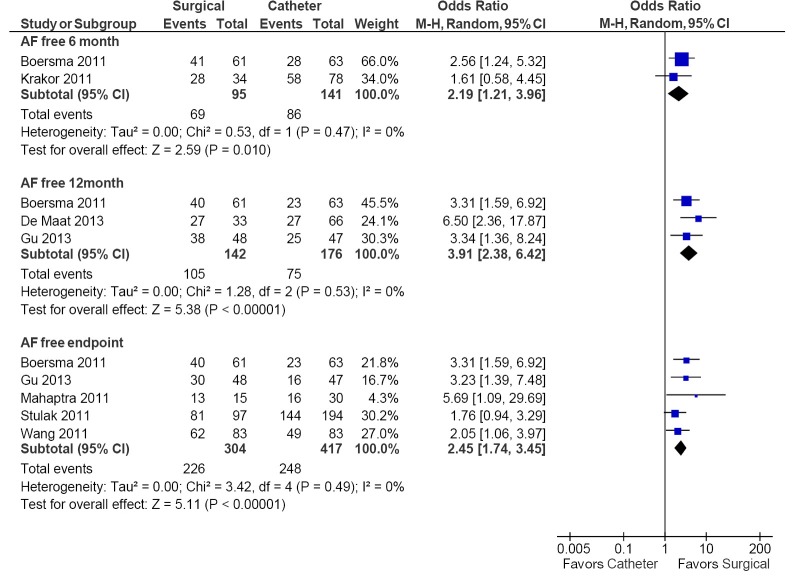
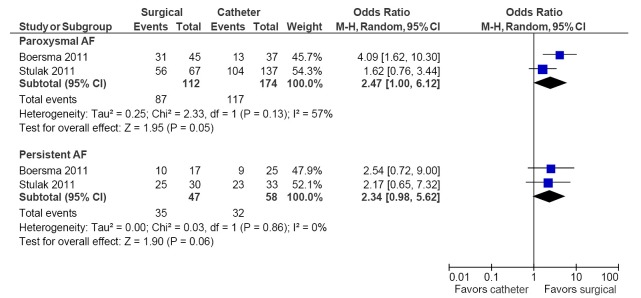
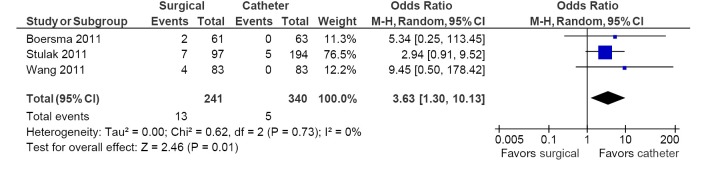
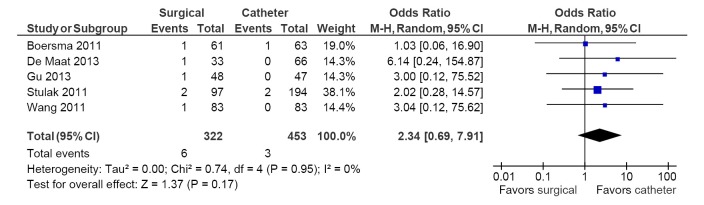
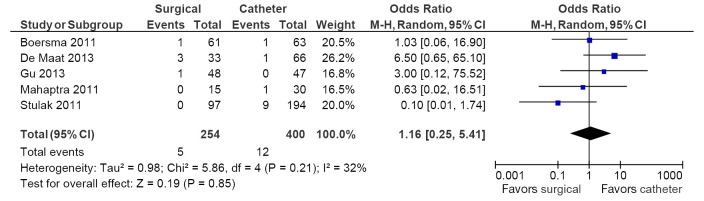
Results: Seven studies were deemed suitable for analysis according to the inclusion criteria. Freedom from AF was significantly higher in the surgical ablation group versus the catheter ablation group at 6-month, 12-month and study endpoint follow-up periods. Subgroup analysis demonstrated similar trends, with higher freedom from AF in the surgical ablation group for paroxysmal AF patients. The incidence of pacemaker implantation was higher, while no difference in stroke or cardiac tamponade was demonstrated for the surgical versus catheter ablation groups.
Conclusions: Current evidence suggests that epicardial ablative strategies are associated with higher freedom from AF, higher pacemaker implantation rates and comparable neurological complications and cardiac tamponade incidence to catheter ablative treatment. Other complications and risks were poorly reported, which warrants further randomized controlled trials (RCTs) of adequate power and follow-up duration.
Keywords: Atrial fibrillation (AF); catheter ablation; endocardial ablation; epicardial ablation; surgical ablation.
Figures
References
-
- European Heart Rhythm Association , European Association for Cardio-Thoracic Surgery, Camm AJ, et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J 2010;31:2369-429 - PubMed
-
- Wilber DJ, Pappone C, Neuzil P, et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA 2010;303:333-40 - PubMed
-
- Calkins H, Reynolds MR, Spector P, et al. Treatment of atrial fibrillation with antiarrhythmic drugs or radiofrequency ablation: two systematic literature reviews and meta-analyses. Circ Arrhythm Electrophysiol 2009;2:349-61 - PubMed
-
- Weerasooriya R, Khairy P, Litalien J, et al. Catheter ablation for atrial fibrillation: are results maintained at 5 years of follow-up? J Am Coll Cardiol 2011;57:160-6 - PubMed
Publication types
LinkOut - more resources
Full Text Sources