

Illustrated techniques for performing the Cox-Maze IV procedure through a right mini-thoracotomy
- PMID: 24516807
- PMCID: PMC3904342
- DOI: 10.3978/j.issn.2225-319X.2013.12.11
Illustrated techniques for performing the Cox-Maze IV procedure through a right mini-thoracotomy
Abstract
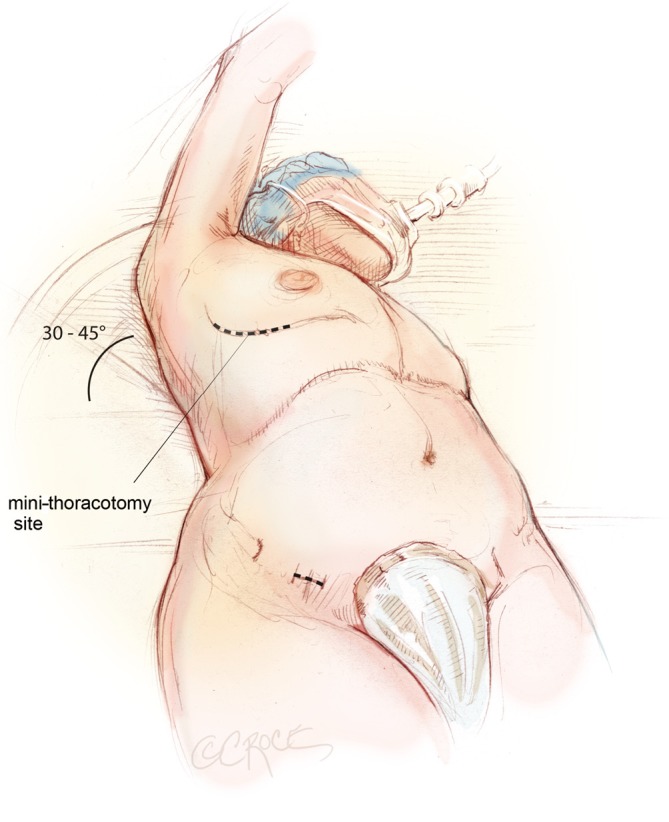
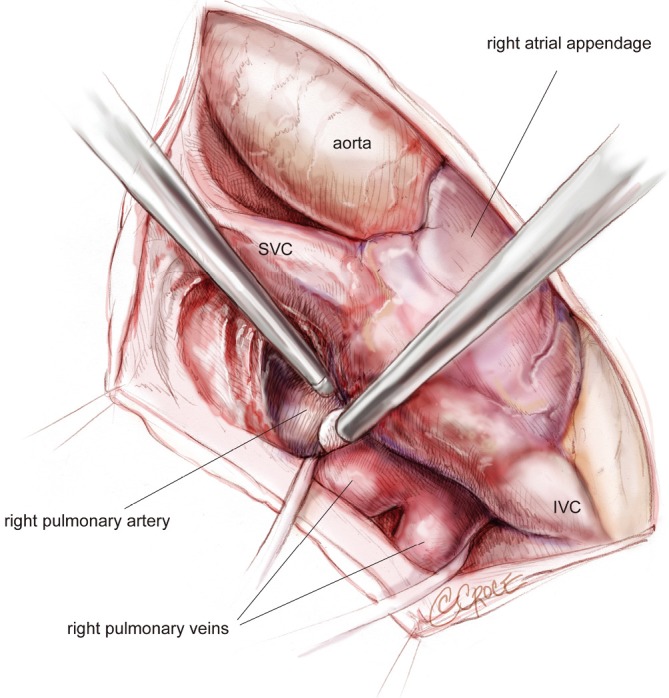
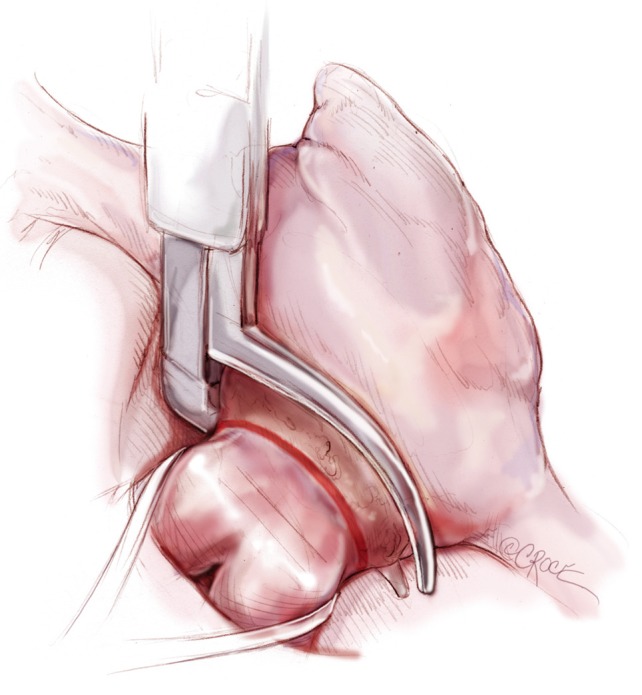
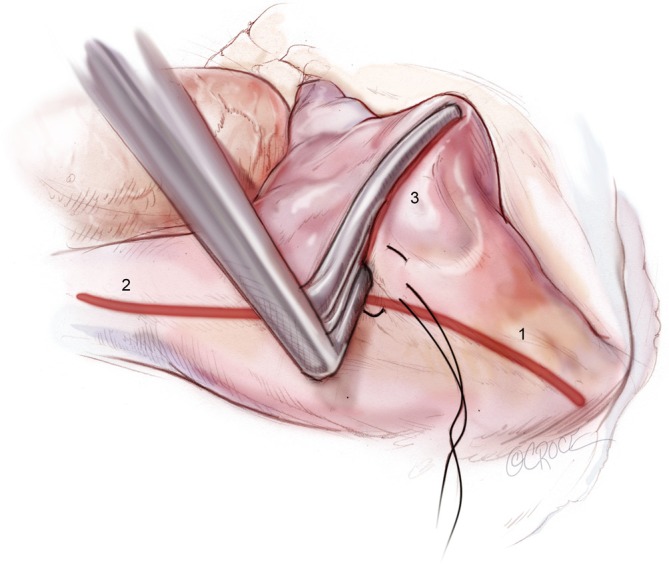
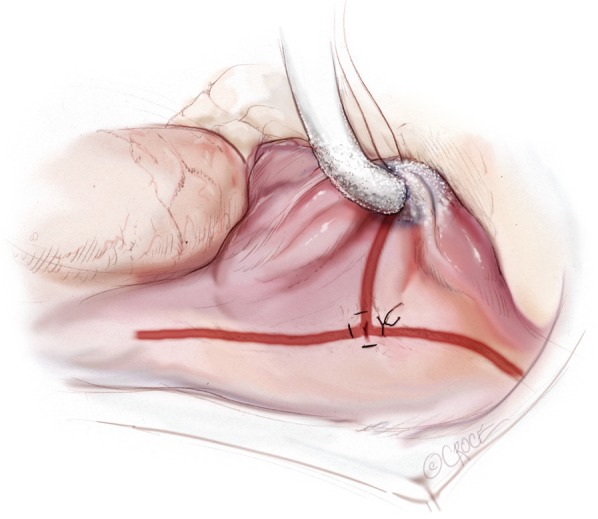
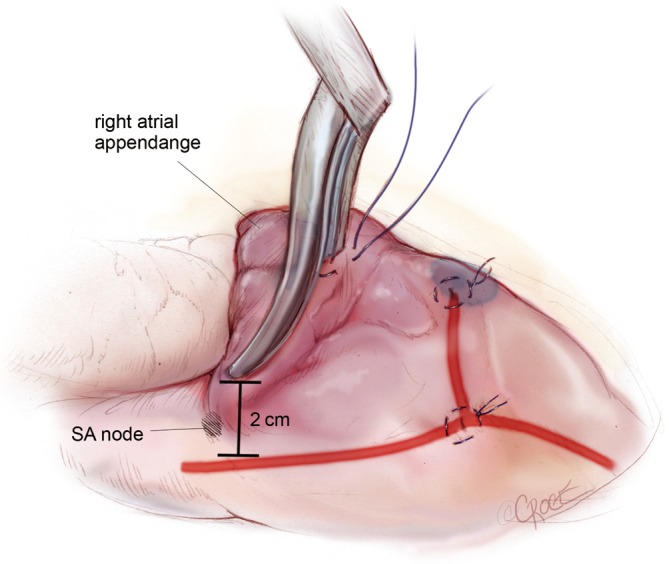
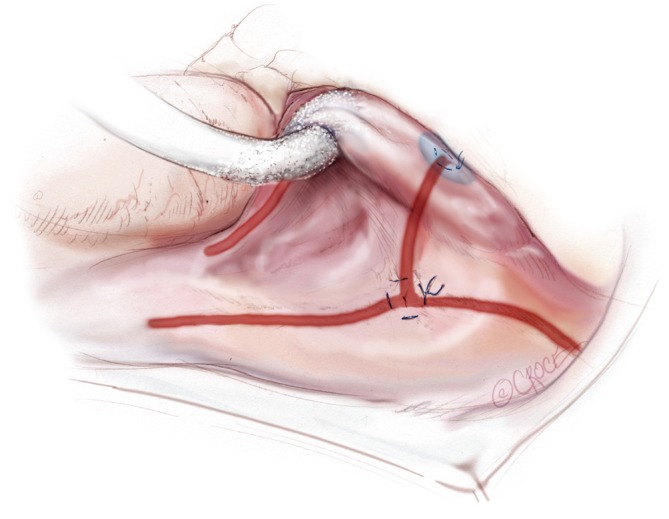
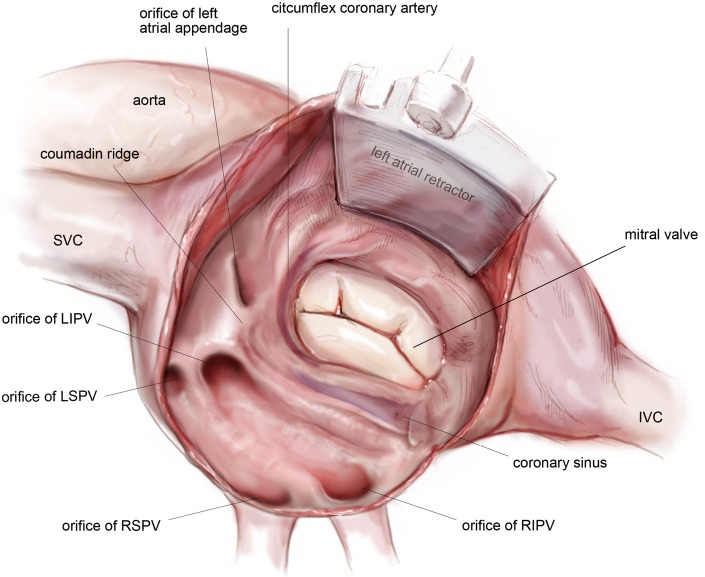
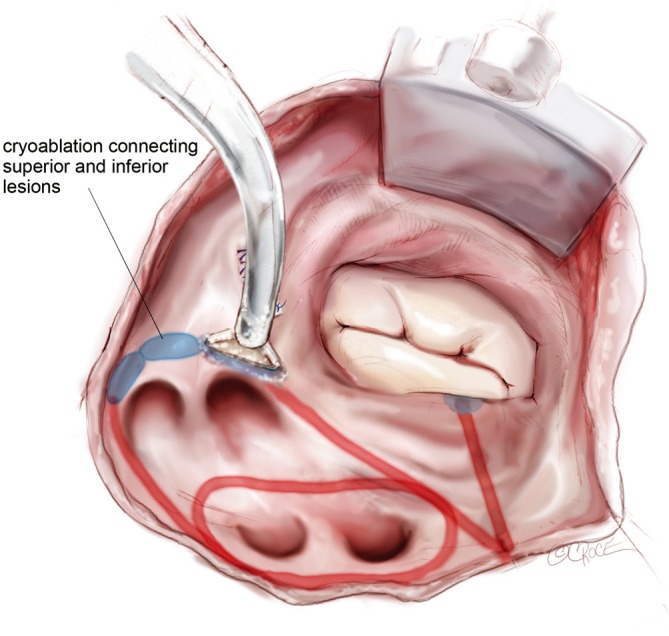
The Cox-Maze IV procedure has replaced the "cut-and-sew" technique of the original Cox-Maze operation with lines of ablation created using bipolar radiofrequency (RF) and cryothermal energy devices. In select patients, this procedure can be performed through a right mini-thoracotomy. This illustrated review is the first to detail the complete steps of the Cox-Maze IV procedure performed through a right mini-thoracotomy with careful attention paid to operative anatomy and advice. Pre- and post-operative management and outcomes are also discussed. This should be a practical guide for the practicing cardiac surgeon.
Keywords: Atrial fibrillation (AF); Cox-Maze IV; right mini-thoracotomy.
Figures
References
-
- Cox JL, Ad N, Palazzo T. Impact of the maze procedure on the stroke rate in patients with atrial fibrillation. J Thorac Cardiovasc Surg 1999;118:833-40 - PubMed
-
- Feinberg MS, Waggoner AD, Kater KM, et al. Restoration of atrial function after the maze procedure for patients with atrial fibrillation. Assessment by Doppler echocardiography. Circulation 1994;90:II285-92 - PubMed
-
- Prasad SM, Maniar HS, Camillo CJ, et al. The Cox maze III procedure for atrial fibrillation: long-term efficacy in patients undergoing lone versus concomitant procedures. J Thorac Cardiovasc Surg 2003;126:1822-8 - PubMed
-
- Gammie JS, Haddad M, Milford-Beland S, et al. Atrial fibrillation correction surgery: lessons from the Society of Thoracic Surgeons National Cardiac Database. Ann Thorac Surg 2008;85:909-14 - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources