

Improving preventive care in high risk children with asthma: lessons learned
- PMID: 24517110
- PMCID: PMC4428172
- DOI: 10.3109/02770903.2014.892608
Improving preventive care in high risk children with asthma: lessons learned
Abstract
Objectives: Rates of preventive asthma care after an asthma emergency department (ED) visit are low among inner-city children. The objective of this study was to test the efficacy of a clinician and caregiver feedback intervention (INT) on improving preventive asthma care following an asthma ED visit compared to an attention control group (CON).
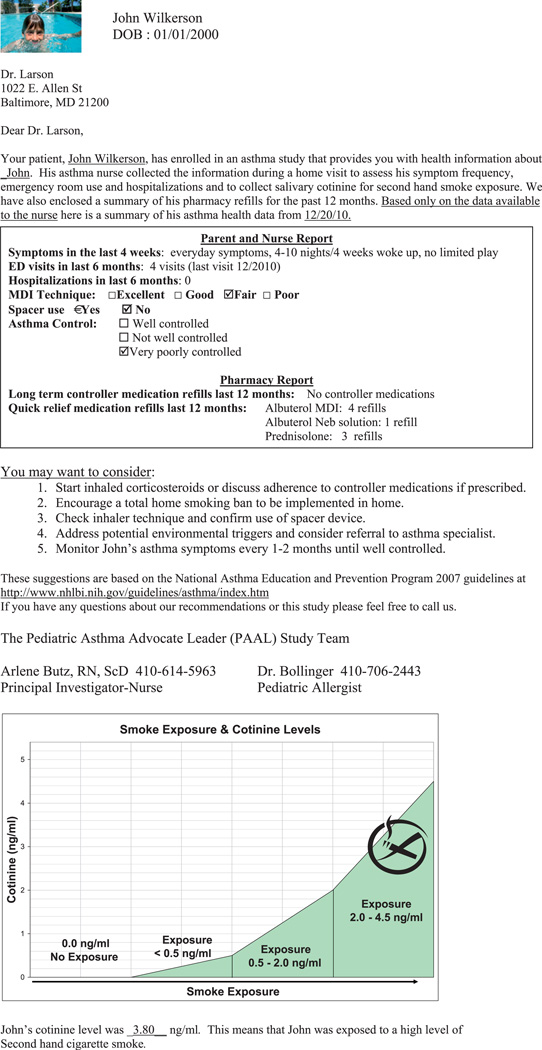
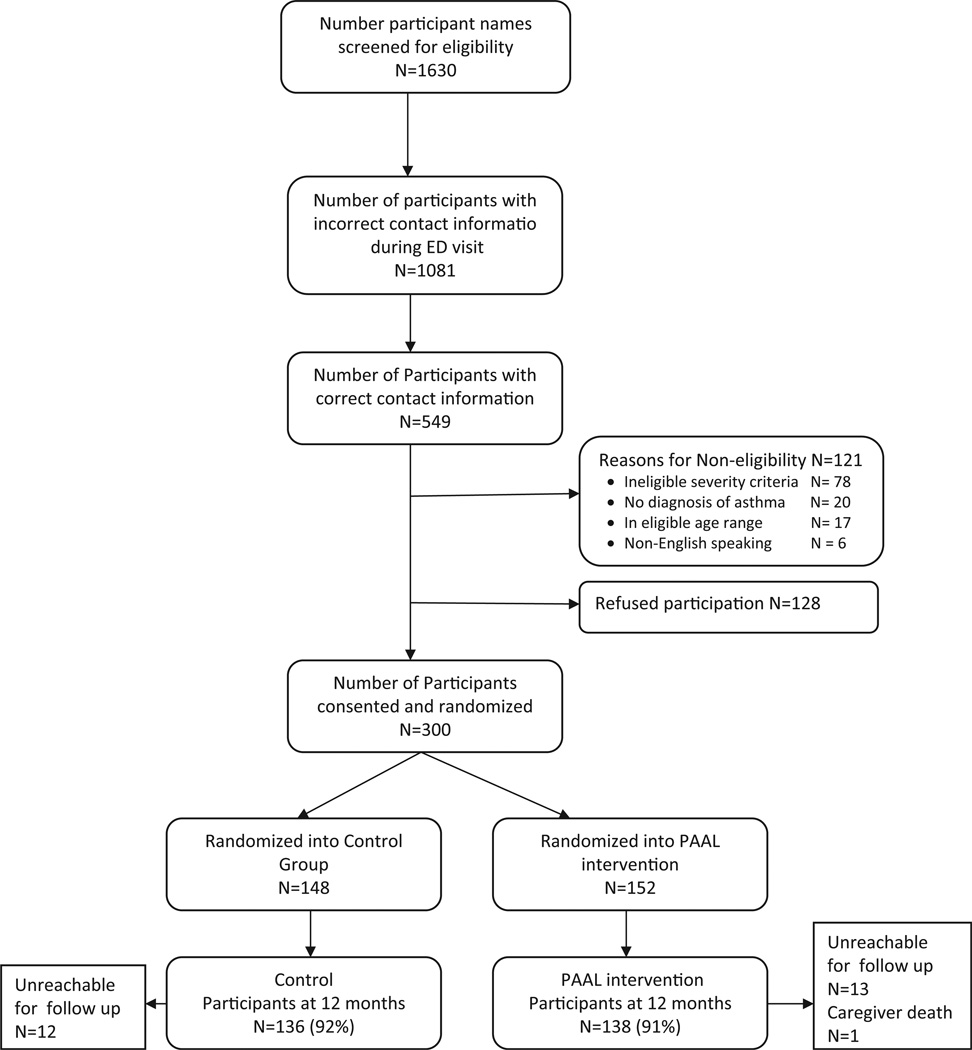
Methods: Children with persistent asthma and recent asthma ED visits (N = 300) were enrolled and randomized into a feedback intervention or an attention control group and followed for 12 months. All children received nurse visits. Data were obtained from interviews, child salivary cotinine levels and pharmacy records. Standard t-test, chi-square and multiple logistic regression tests were used to test for differences between the groups for reporting greater than or equal to two primary care provider (PCP) preventive care visits for asthma over 12 months.
Results: Children were primarily male, young (3-5 years), African American and Medicaid insured. Mean ED visits over 12 months was high (2.29 visits). No difference by group was noted for attending two or more PCP visits/12 months or having an asthma action plan (AAP). Children having an AAP at baseline were almost twice as likely to attend two or more PCP visits over 12 months while controlling for asthma control, group status, child age and number of asthma ED visits.
Conclusions: A clinician and caregiver feedback intervention was unsuccessful in increasing asthma preventive care compared to an attention control group. Further research is needed to develop interventions to effectively prevent morbidity in high risk inner-city children with frequent ED utilization.
Trial registration: ClinicalTrials.gov NCT00860418.
Keywords: Management/control; pediatrics; prevention.
Conflict of interest statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Figures
References
-
- Bloom B, Dey AN. Summary health statistics for U.S. children: National Health Interview Survey 2004. National Center for Health Statistics. Vital Health Stat. 2006;10:4–5. - PubMed
-
- Akinbami LJ, Moorman JE, Bailey C, Zahran HS, King M, Johnson CA, Liu X. Trends in asthma prevalence, health care use and mortality in the United States, 2001–2010. NCHS Data Brief. 2012;94:1–7. - PubMed
-
- Akinbami LJ, Moorman JE, Garbe PL, Sondik EJ. Status of childhood asthma in the United States, 1980–2007. Pediatrics. 2009;123:S131–S145. - PubMed
-
- Centers for Disease Control. National Surveillance for Asthma – United States 1980–2004. MMWR. 2007;56:1–14. - PubMed
-
- USDHHS. The National Asthma Education and Prevention Program. Expert panel report 3 (EPR3): guidelines for the diagnosis and management of asthma. 2007 NIH Publication No. 07-4051. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous