

Risk and prognosis of ovarian cancer in women with endometriosis: a meta-analysis
- PMID: 24518590
- PMCID: PMC3974076
- DOI: 10.1038/bjc.2014.29
Risk and prognosis of ovarian cancer in women with endometriosis: a meta-analysis
Abstract
Background: The risk and prognosis of ovarian cancer have not been well established in women with endometriosis. Thus, we investigated the impact of endometriosis on the risk and prognosis for ovarian cancer, and evaluated clinicopathologic characteristics of endometriosis-associated ovarian cancer (EAOC) in comparison with non-EAOC.
Methods: After we searched an electronic search to identify relevant studies published online between January 1990 and December 2012, we found 20 case-control and 15 cohort studies including 444,255 patients from 1,625 potentially relevant studies. In the meta-analysis, ovarian cancer risk by endometriosis and clinicopathologic characteristics were evaluated using risk ratio (RR) or standard incidence ratio (SIR), and prognosis was investigated using hazard ratio (HR) with 95% confidence interval (CI). Heterogeneity was evaluated using Higgins I(2) to select fixed-effect (I(2) ≤50%) or random effects models (I(2)>50%), and found no publication bias using funnel plots with Egger's test (P>0.05). Furthermore, we performed subgroup analyses based on study design, assessment of endometriosis, histology, disease status, quality of study and adjustment for potential confounding factors to minimise bias.
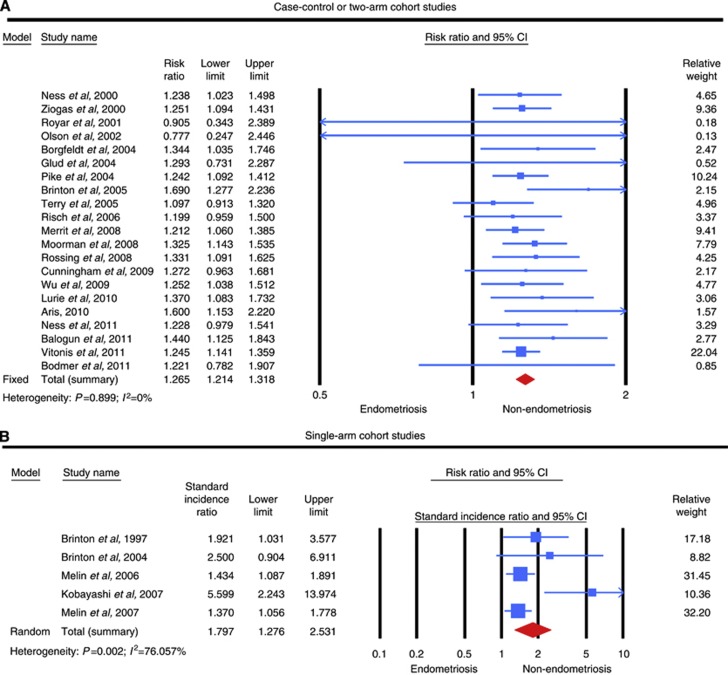
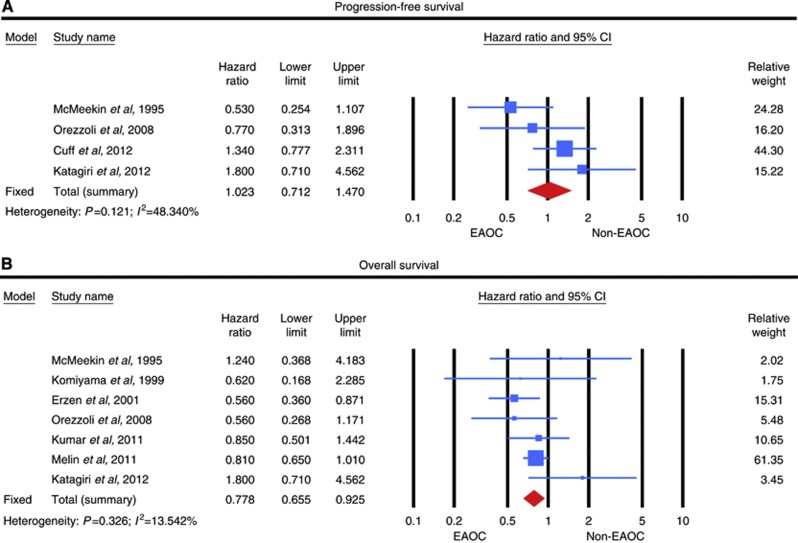
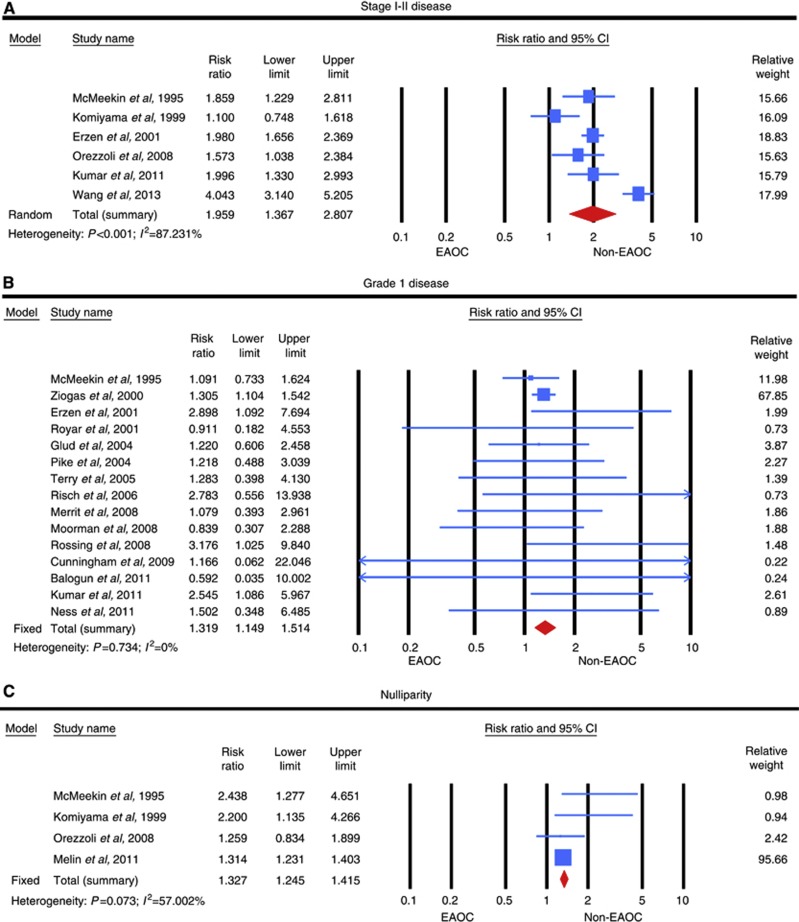
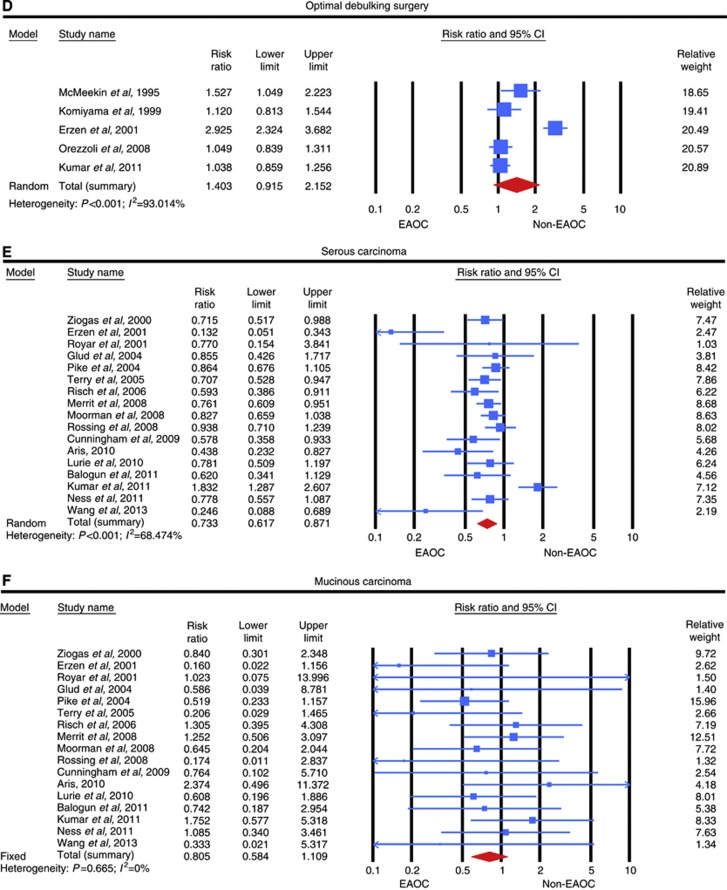
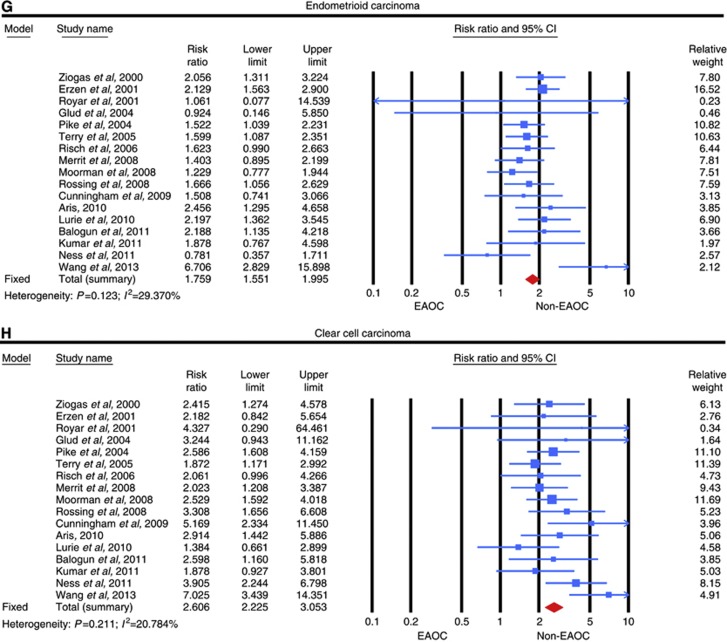
Results: Endometriosis increased ovarian cancer risk in case-control or two-arm cohort studies (RR, 1.265; 95% CI, 1.214-1.318) and single-arm cohort studies (SIR, 1.797; 95% CI, 1.276-2.531), which were similar in subgroup analyses. Although progression-free survival was not different between EAOC and non-EAOC (HR, 1.023; 95% CI, 0.712-1.470), EAOC was associated with better overall survival than non-EAOC in crude analyses (HR, 0.778; 95% CI, 0.655-0.925). However, progression-free survival and overall survival were not different between the two groups in subgroup analyses. Stage I-II disease, grade 1 disease and nulliparity were more common in EAOC (RRs, 1.959, 1.319 and 1.327; 95% CIs, 1.367-2.807, 1.149-1.514 and 1.245-1.415), whereas probability of optimal debulking surgery was not different between the two groups (RR, 1.403; 95% CI, 0.915-2.152). Furthermore, endometrioid and clear cell carcinomas were more common in EAOC (RRs, 1.759 and 2.606; 95% CIs, 1.551-1.995 and 2.225-3.053), whereas serous carcinoma was less frequent in EAOC than in non-EAOC (RR, 0.733; 95% CI, 0.617-0.871), and there was no difference in the risk of mucinous carcinoma between the two groups (RR, 0.805; 95% CI, 0.584-1.109). These clinicopathologic characteristics were also similar in subgroup analyses.
Conclusions: Endometriosis is strongly associated with the increased risk of ovarian cancer, and EAOC shows favourable characteristics including early-stage disease, low-grade disease and a specific histology such as endometrioid or clear cell carcinoma. However, endometriosis may not affect disease progression after the onset of ovarian cancer.
Figures
References
-
- Balogun N, Gentry-Maharaj A, Wozniak EL, Lim A, Ryan A, Ramus SJ, Ford J, Burnell M, Widschwendter M, Gessler SF, Gayther SA, Jacobs IJ, Menon U. Recruitment of newly diagnosed ovarian cancer patients proved challenging in a multicentre biobanking study. J Clin Epidemiol. 2011;64:525–530. - PubMed
-
- Bodmer M, Becker C, Meier C, Jick SS, Meier CR. Use of metformin and the risk of ovarian cancer: a case-control analysis. Gynecol Oncol. 2011;123:200–204. - PubMed
-
- Borgfeldt C, Andolf E. Cancer risk after hospital discharge diagnosis of benign ovarian cysts and endometriosis. Acta Obstet Gynecol Scand. 2004;83:395–400. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
