

Carcinoma ex-Schneiderian papilloma (malignant transformation): a clinicopathologic and immunophenotypic study of 20 cases combined with a comprehensive review of the literature
- PMID: 24519376
- PMCID: PMC4126921
- DOI: 10.1007/s12105-014-0527-7
Carcinoma ex-Schneiderian papilloma (malignant transformation): a clinicopathologic and immunophenotypic study of 20 cases combined with a comprehensive review of the literature
Abstract
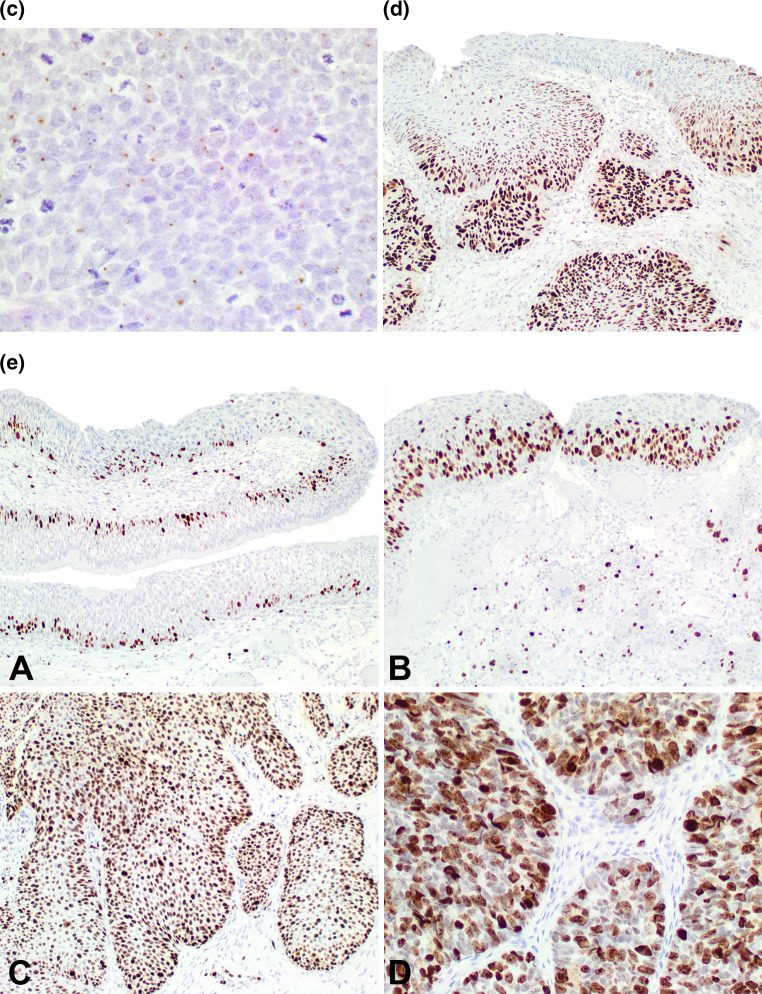
Schneiderian papilloma (SP) are uncommon tumors with malignant transformation even less common. The histologic criteria to define malignant transformation are not well developed nor is the immunohistochemical profile reported in a large series of carcinomas. 20 cases of malignant transformation of SP included 7 females and 13 males, aged 38-86 years (mean 60.7 years). Patients presented most frequently with a mass (n = 11) and obstructive symptoms (n = 7), present for 38.7 months (mean). Most patients had no previous history of SP (n = 13); metachronous carcinoma was identified in 7 patients an average of 34.4 months after the first diagnosis of SP, with 1-4 recurrences of SP. With a mean size of 4.1 cm, the majority of tumors involved a combination of more than one anatomic site (n = 10), followed by the maxillary sinus only (n = 5) or nasal cavity only (n = 3). Histologically, 17 were inverted and 3 exophytic type SP. There were 17 squamous cell carcinomas, 2 mucoepidermoid carcinomas and 1 sinonasal undifferentiated carcinoma, comprising from 10 to 95 % of the tumor volume. Malignant histologic features included atypical mitoses, necrosis, bone invasion, lymphovascular invasion, decreased transmigrating neutrophils, paradoxical maturation, dyskeratosis and/or perineural invasion (n = 3). Patients tended to present with advanced stage (n = 14, Stage III and IV). Immunohistochemical studies showed positive reactions in the malignancies for CK5/6 (86 %), p63 (86 %), CK7 (luminal, 50 %), p53 (83 %), and p16 (25 %). In situ hybridization detected human papillomavirus in 26 %. Surgery was often accompanied by radiation therapy (n = 13), with a mean of 2.4 years of follow-up. Five patients developed a recurrence between 0.8 and 3.3 years. Carcinomas ex-SP are less common and are associated with better outcome than previously reported. Patients tend to present with a synchronous carcinoma, developing in an inverted type SP, with squamous cell carcinoma the most common malignancy. Development of metachronous carcinomas ex-SP was always preceded by SP recurrence in this series.
Figures





References
-
- AJCC Cancer Staging Manual, 7th ed. New York: Springer; 2009.
-
- Buchwald C, Franzmann MB, Jacobsen GK, Juhl BR, Lindeberg H. Carcinomas occurring in papillomas of the nasal septum associated with human papilloma virus (HPV) Rhinology. 1997;35:74–78. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
