

Twenty five year follow-up for breast cancer incidence and mortality of the Canadian National Breast Screening Study: randomised screening trial
- PMID: 24519768
- PMCID: PMC3921437
- DOI: 10.1136/bmj.g366
Twenty five year follow-up for breast cancer incidence and mortality of the Canadian National Breast Screening Study: randomised screening trial
Abstract
Objective: To compare breast cancer incidence and mortality up to 25 years in women aged 40-59 who did or did not undergo mammography screening.
Design: Follow-up of randomised screening trial by centre coordinators, the study's central office, and linkage to cancer registries and vital statistics databases.
Setting: 15 screening centres in six Canadian provinces,1980-85 (Nova Scotia, Quebec, Ontario, Manitoba, Alberta, and British Columbia).
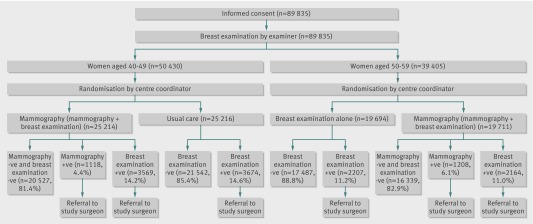
Participants: 89,835 women, aged 40-59, randomly assigned to mammography (five annual mammography screens) or control (no mammography).
Interventions: Women aged 40-49 in the mammography arm and all women aged 50-59 in both arms received annual physical breast examinations. Women aged 40-49 in the control arm received a single examination followed by usual care in the community.
Main outcome measure: Deaths from breast cancer.
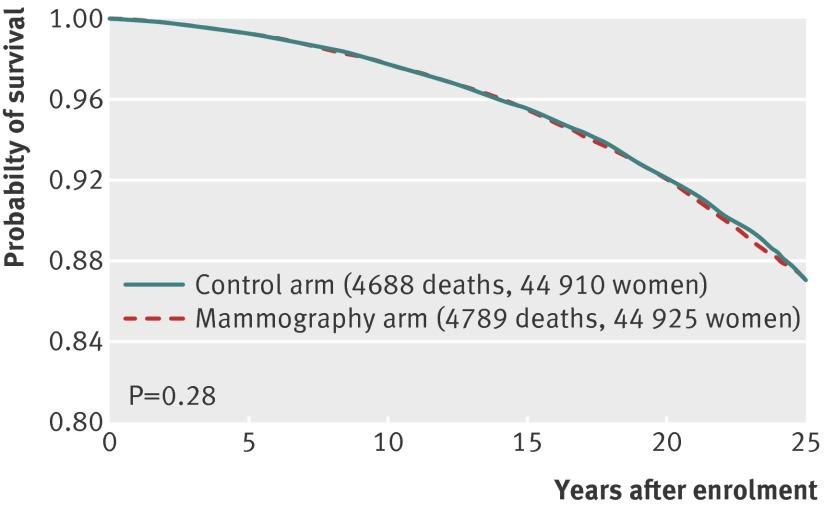
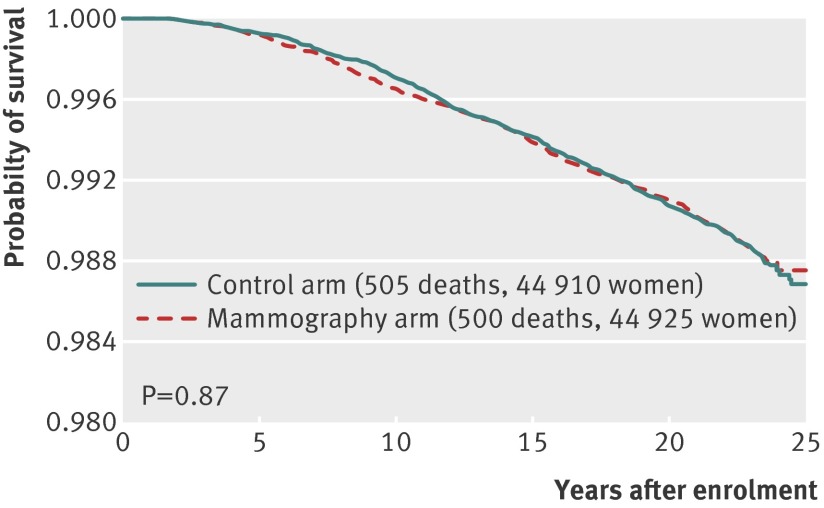
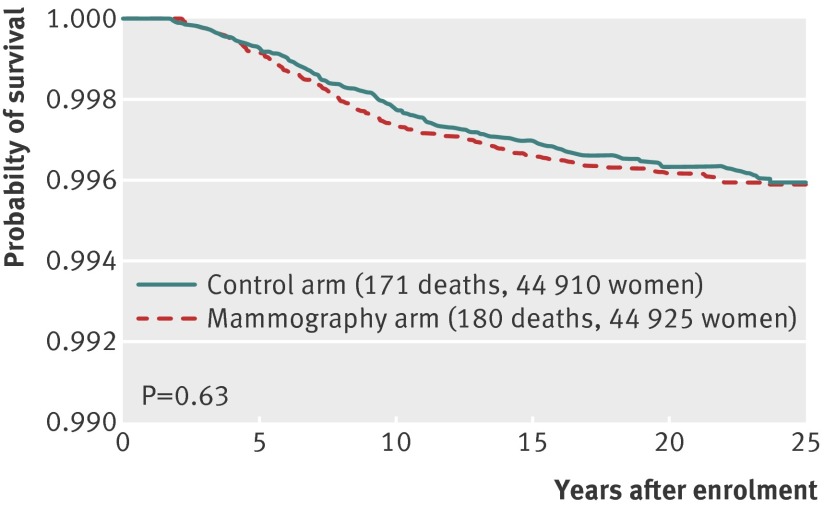
Results: During the five year screening period, 666 invasive breast cancers were diagnosed in the mammography arm (n=44,925 participants) and 524 in the controls (n=44,910), and of these, 180 women in the mammography arm and 171 women in the control arm died of breast cancer during the 25 year follow-up period. The overall hazard ratio for death from breast cancer diagnosed during the screening period associated with mammography was 1.05 (95% confidence interval 0.85 to 1.30). The findings for women aged 40-49 and 50-59 were almost identical. During the entire study period, 3250 women in the mammography arm and 3133 in the control arm had a diagnosis of breast cancer, and 500 and 505, respectively, died of breast cancer. Thus the cumulative mortality from breast cancer was similar between women in the mammography arm and in the control arm (hazard ratio 0.99, 95% confidence interval 0.88 to 1.12). After 15 years of follow-up a residual excess of 106 cancers was observed in the mammography arm, attributable to over-diagnosis.
Conclusion: Annual mammography in women aged 40-59 does not reduce mortality from breast cancer beyond that of physical examination or usual care when adjuvant therapy for breast cancer is freely available. Overall, 22% (106/484) of screen detected invasive breast cancers were over-diagnosed, representing one over-diagnosed breast cancer for every 424 women who received mammography screening in the trial.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Too much mammography.BMJ. 2014 Feb 11;348:g1403. doi: 10.1136/bmj.g1403. BMJ. 2014. PMID: 24519765 No abstract available.
-
The Canadian National Breast Screening Study: caveat emptor.AJR Am J Roentgenol. 2014 May;202(5):W505. doi: 10.2214/AJR.14.12722. AJR Am J Roentgenol. 2014. PMID: 24758687 No abstract available.
-
Fifty years of age-based screening: time for a new risk-based screening approach.Evid Based Med. 2014 Oct;19(5):183. doi: 10.1136/eb-2014-101798. Epub 2014 May 1. Evid Based Med. 2014. PMID: 24785471 No abstract available.
-
ACP Journal Club. Annual mammography screening did not reduce long-term breast cancer mortality in women 40 to 59 years of age.Ann Intern Med. 2014 May 20;160(10):JC7. doi: 10.7326/0003-4819-160-10-201405200-02007. Ann Intern Med. 2014. PMID: 24842441 No abstract available.
-
Re: "Twenty five year follow-up for breast cancer incidence and mortality of the Canadian National Breast Screening Study: randomised screening trial".Am J Epidemiol. 2014 Oct 1;180(7):759-60. doi: 10.1093/aje/kwu227. Epub 2014 Sep 5. Am J Epidemiol. 2014. PMID: 25194149 No abstract available.
-
The authors reply.Am J Epidemiol. 2014 Oct 1;180(7):760-1. doi: 10.1093/aje/kwu228. Epub 2014 Sep 5. Am J Epidemiol. 2014. PMID: 25194150 No abstract available.
-
Screening mammography may be less effective than thought.J Midwifery Womens Health. 2014 Jul-Aug;59(4):465-7. doi: 10.1111/jmwh.12215_1. J Midwifery Womens Health. 2014. PMID: 25215355 No abstract available.
-
Reply to Kopans.Breast Cancer Res Treat. 2017 Nov;166(2):653-654. doi: 10.1007/s10549-017-4465-4. Epub 2017 Aug 30. Breast Cancer Res Treat. 2017. PMID: 28856529 No abstract available.
-
Rebuttal comments.Breast Cancer Res Treat. 2017 Nov;166(2):655-656. doi: 10.1007/s10549-017-4471-6. Epub 2017 Sep 16. Breast Cancer Res Treat. 2017. PMID: 28918479 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical