

Disulfiram efficacy in the treatment of alcohol dependence: a meta-analysis
- PMID: 24520330
- PMCID: PMC3919718
- DOI: 10.1371/journal.pone.0087366
Disulfiram efficacy in the treatment of alcohol dependence: a meta-analysis
Abstract
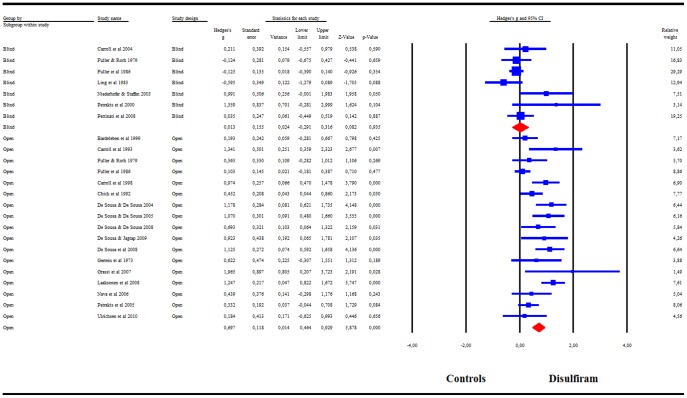
Background: Despite its success with compliant or supervised patients, disulfiram has been a controversial medication in the treatment of alcoholism. Often, study designs did not recognize a pivotal factor in disulfiram research, the importance of an open-label design. Our objectives are: (1) to analyze the efficacy and safety of disulfiram in RCTs in supporting abstinence and (2) to compare blind versus open-label studies, hypothesizing that blinded studies would show no difference between disulfiram and control groups because the threat would be evenly spread across all groups.
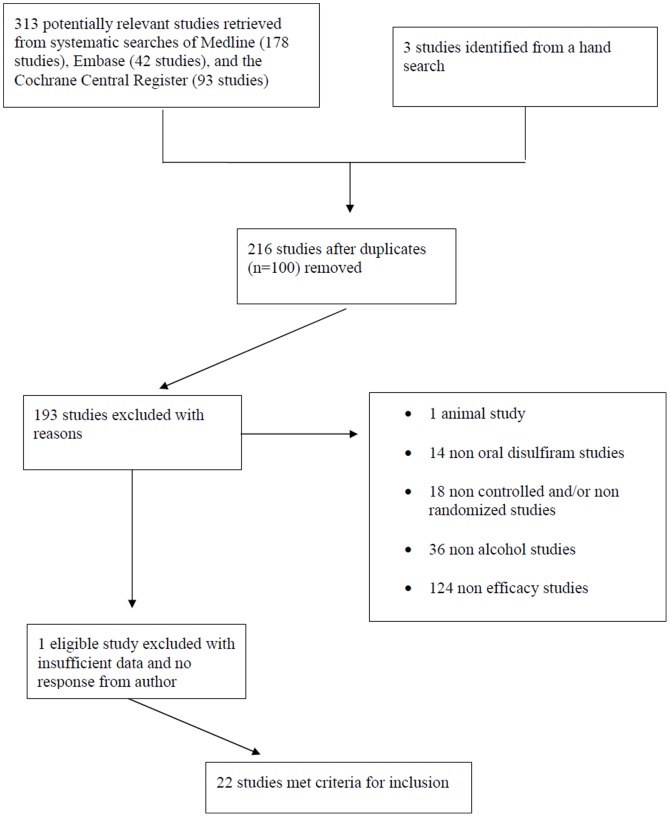
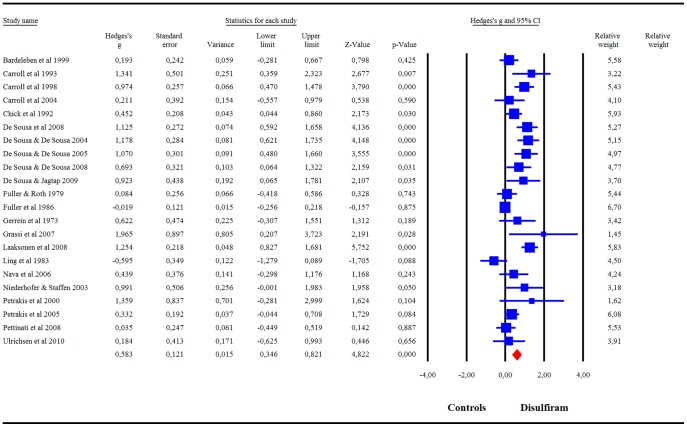
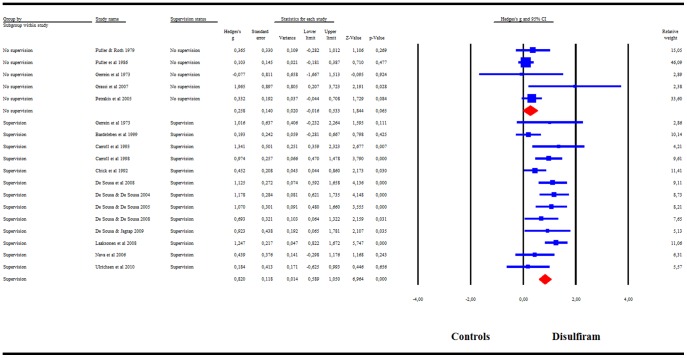
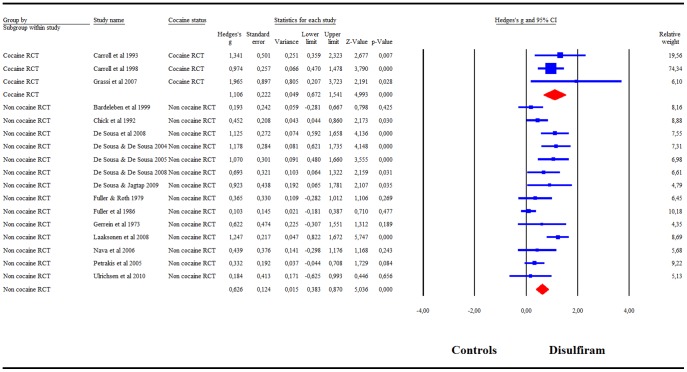
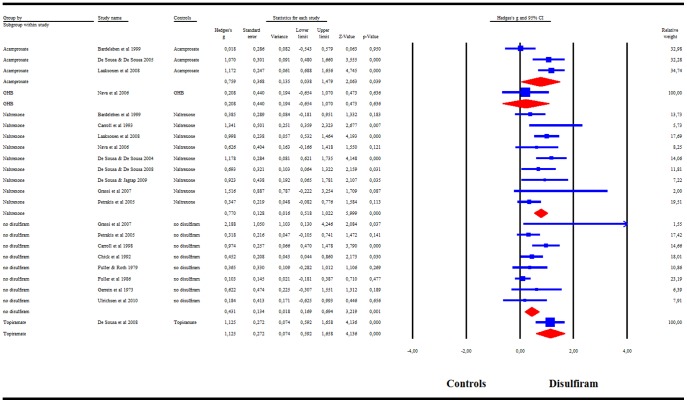
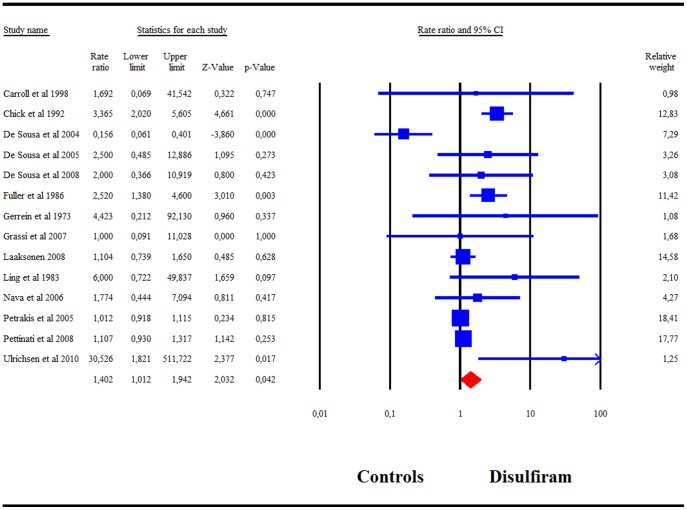
Methods and findings: We searched PubMed, EMBASE and the Cochrane Central Register for RCTs on disulfiram use with alcoholics in comparison to any alcoholic control group. The primary outcome was defined by the authors of each trial. Additional analyses included: blind vs. open-label, with or without supervision, cocaine study or not, and type of control. Overall, the 22 included studies showed a higher success rate of disulfiram compared to controls Hedges'g = .58 (95%CI = .35-.82). When comparing blind and open-label RCTs, only open-label trials showed a significant superiority over controls g = .70 (95%CI = .46-.93). RCTs with blind designs showed no efficacy of disulfiram compared to controls. Disulfiram was also more effective than the control condition when compared to naltrexone g = .77, 95%CI = .52-1.02, to acamprosate g = .76, 95%CI = .04-1.48, and to the no disulfiram groups g = .43, 95%CI = .17-.69. LIMITS INCLUDE: (1) a population of 89% male subjects and (2) a high but unavoidable heterogeneity of the studies with a substantial I-square in most subgroups of studies.
Conclusions: Blinded studies were incapable of distinguishing a difference between treatment groups and thus are incompatible with disulfiram research. Based on results with open-label studies, disulfiram is a safe and efficacious treatment compared to other abstinence supportive pharmacological treatments or to no disulfiram in supervised studies for problems of alcohol abuse or dependence.
Conflict of interest statement
Figures
References
-
- Azrin NH, Sisson RW, Meyers R, Godley M (1982) Alcoholism treatment by disulfiram and community reinforcement therapy. J Behav Ther Exp Psychiatry 13: 105–112. - PubMed
-
- Brewer C, Meyers R, Johnson J (2000) Does disulfiram help to prevent relapse in alcohol abuse? CNS Drugs 14: 329–341.
-
- Wright C, Moore RD (1990) Disulfiram treatment of alcoholism. Am J Med 88: 647–655. - PubMed
-
- Wilson A, Blanchard R, Davidson W, McRae L, Maini K (1984) Disulfiram implantation: a dose response trial. J Clin Psychiatry 45: 242–247. - PubMed
-
- Fuller R, Gordis E (2004) Does disulfiram have a role in alcoholism treatment today? Addiction 99: 21–24. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
