

Asymptomatic ratio for seasonal H1N1 influenza infection among schoolchildren in Taiwan
- PMID: 24520993
- PMCID: PMC3938038
- DOI: 10.1186/1471-2334-14-80
Asymptomatic ratio for seasonal H1N1 influenza infection among schoolchildren in Taiwan
Abstract
Background: Studies indicate that asymptomatic infections do indeed occur frequently for both seasonal and pandemic influenza, accounting for about one-third of influenza infections. Studies carried out during the 2009 pH1N1 pandemic have found significant antibody response against seasonal H1N1 and H3N2 vaccine strains in schoolchildren receiving only pandemic H1N1 monovalent vaccine, yet reported either no symptoms or only mild symptoms.
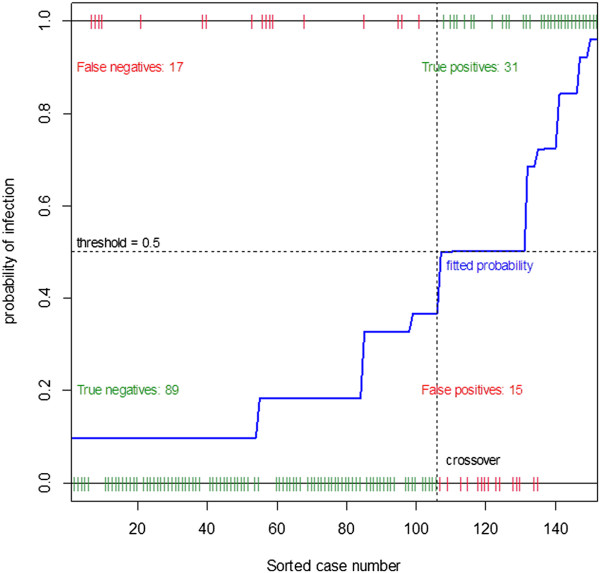
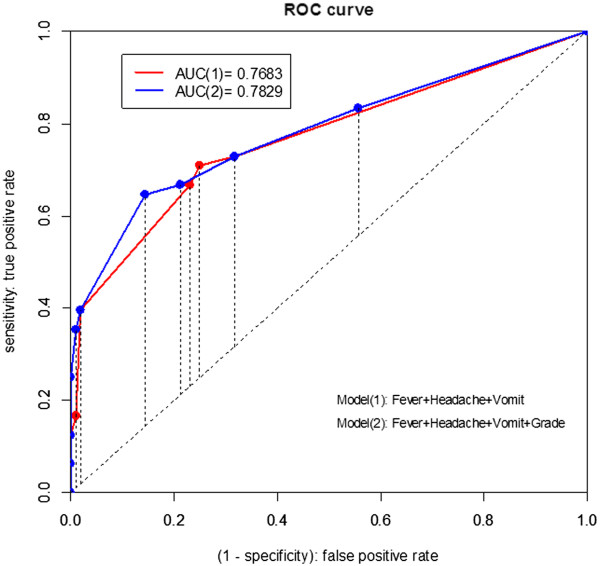
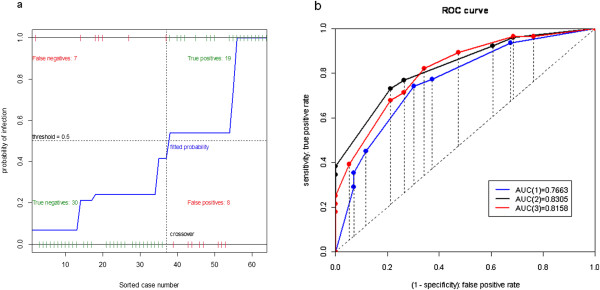
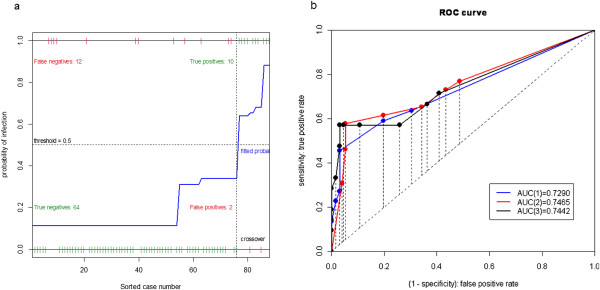
Methods: Serum samples of 255 schoolchildren, who had not received vaccination and had pre-season HI Ab serotiters <40, were collected from urban, rural areas and an isolated island in Taiwan during the 2005-2006 influenza season. Their hemagglutination inhibition antibody (HI Ab) serotiters against the 2005 A/New Caledonia/20/99 (H1N1) vaccine strain at pre-season and post-season were measured to determine the symptoms with the highest correlation with infection, as defined by 4-fold rise in HI titer. We estimate the asymptomatic ratio, or the proportion of asymptomatic infections, for schoolchildren during the 2005-6 influenza season when this vaccine strain was found to be antigenically related to the circulating H1N1 strain.
Results: Fever has the highest correlation with the 2005-06 seasonal influenza A(H1N1) infection, followed by headache, cough, vomiting, and sore throat. Asymptomatic ratio for the schoolchildren is found to range between 55.6% (95% CI: 44.7-66.4)-77.9% (68.8-87.0) using different sets of predictive symptoms. Moreover, the asymptomatic ratio was 66.9% (56.6-77.2) when using US-CDC criterion of fever + (cough/sore throat), and 73.0 (63.3-82.8) when under Taiwan CDC definition of Fever + (cough or sore throat or nose) + ( headache or pain or fatigue).
Conclusions: Asymptomatic ratio for children is found to be substantially higher than that of the general population in literature. In providing reasonable quantification of the asymptomatic infected children spreading pathogens to others in a seasonal epidemic or a pandemic, our estimates of symptomatic ratio of infected children has important clinical and public health implications.
Figures
References
-
- Fox JP, Hall CE, Cooney MK, Foy HM. Influenza virus infections in Seattle families, 1975–1979. I. Study design, methods and the occurrence of infections by time and age. Am J Epidemiol. 1982;14(2):212–227. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
