

Caregiver burden and its determinants among family members of patients with chronic viral hepatitis in Shanghai, China: a community-based survey
- PMID: 24521097
- PMCID: PMC3927630
- DOI: 10.1186/1471-2334-14-82
Caregiver burden and its determinants among family members of patients with chronic viral hepatitis in Shanghai, China: a community-based survey
Abstract
Background: In China, caregivers of chronic viral hepatitis patients experience considerable burdens, stress and disruption of their own well-being and social activities. Measurement of the effect on caregivers is an under-researched area. The Family Burden Interview Schedule (FBIS) was primarily devised for the caregivers of schizophrenia patients, and the adverse effect of the disease was similar to the effect of chronic viral hepatitis on family caregivers. In this study, we prospectively evaluated the psychometric properties of FBIS in the field of chronic viral hepatitis and used it to determine the factors affecting the caregiver burden on the family members of chronic viral hepatitis patients in Shanghai, China.
Methods: A representative sample of patients (n = 1478) and caregivers (n = 1478) was randomly obtained through a multi-stage cluster sampling in Shanghai, China. Reliability and validity tests were used to verify the psychometric properties of the instrument. The two-level random intercept model was applied to determine the factors of the caregiver burden between the household and the community level.
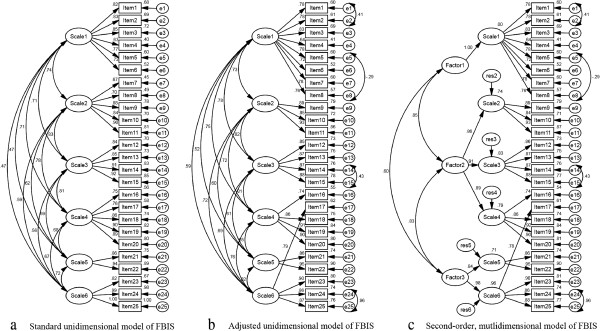
Results: Cronbach's alpha coefficient was 0.90 for the overall instrument with statistical significance. Factor analysis suggested a three-factor model for the FBIS and confirmed that the adjusted unidimensional model and the second-order multidimensional model had better fit statistics. The average score of the caregiver burden in Shanghai was 12.62 ± 10.74, and financial burden constituted the major effect. The two-level random intercept model demonstrated that the risk factors were hospitalisation (β 1.69, 95%CI 0.48 to 2.90), elevated serum alanine aminotransferase levels (β 1.05, 95%CI 0.15 to 1.95), HCV infection (β 4.49, 95%CI 1.22 to 7.77), and acceptance of the hepatitis B vaccine (β 2.20, 95%CI 0.56 to 3.85), whereas the protective factors were no consumption of alcohol (β -2.69, 95%CI -5.19 to -0.19), average monthly costs for patients less than or equal to 100 US dollars (β -2.96, 95%CI -5.83 to -0.09), and good health status of family caregivers (β -9.91, 95%CI -12.76 to -7.05).
Conclusions: FBIS can accurately measure the caregiver burden for chronic hepatitis. Targeting interventions toward the conditions associated with the caregiver burden is of great importance.
Figures
References
-
- Lavanchy D. Worldwide epidemiology of HBV infection, disease burden, and vaccine prevention. J Clin Virol. 2005;14(Suppl):S1–S3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
