

Osteotomy at the distal third of tibial tuberosity with LCP L-buttress plate for correction of tibia vara
- PMID: 24521174
- PMCID: PMC3937034
- DOI: 10.1186/1749-799X-9-9
Osteotomy at the distal third of tibial tuberosity with LCP L-buttress plate for correction of tibia vara
Abstract
Background: Many osteotomy methods and fixation types have been used to correct the misalignment observed in tibia vara and to achieve a more uniform distribution of weight across the knee joint.
Purpose: The aim of this study is to test the efficacy and safety of a modified closing wedge high tibial osteotomy (CWHTO) procedure for tibia vara.
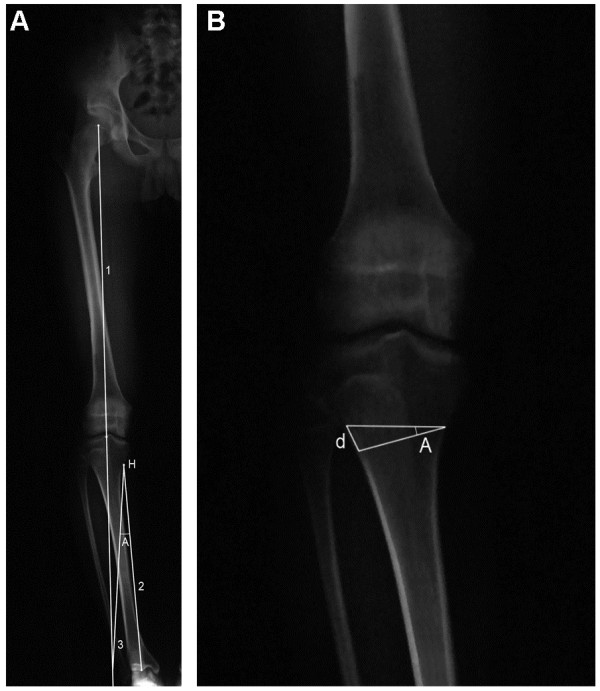
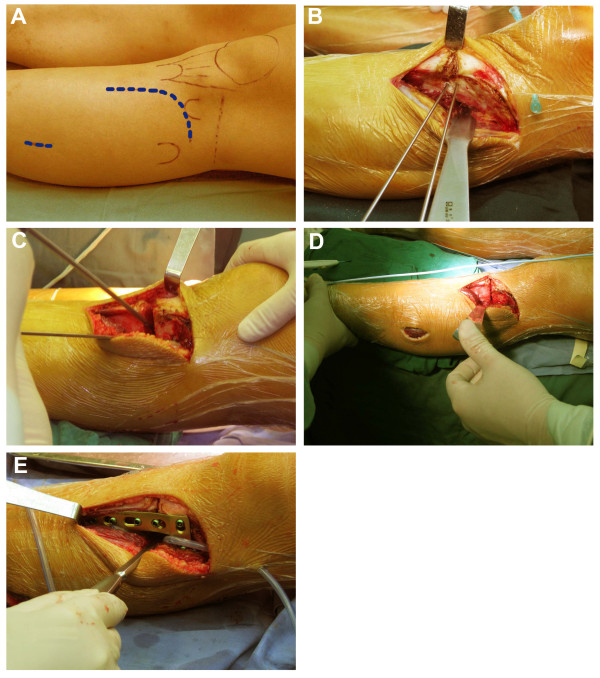
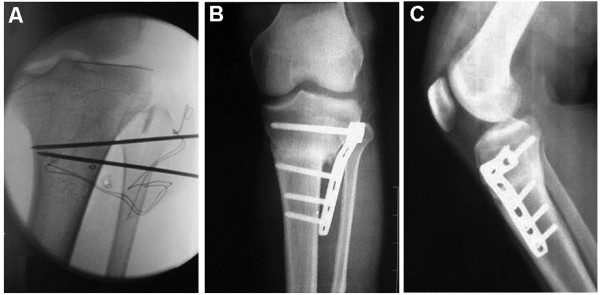
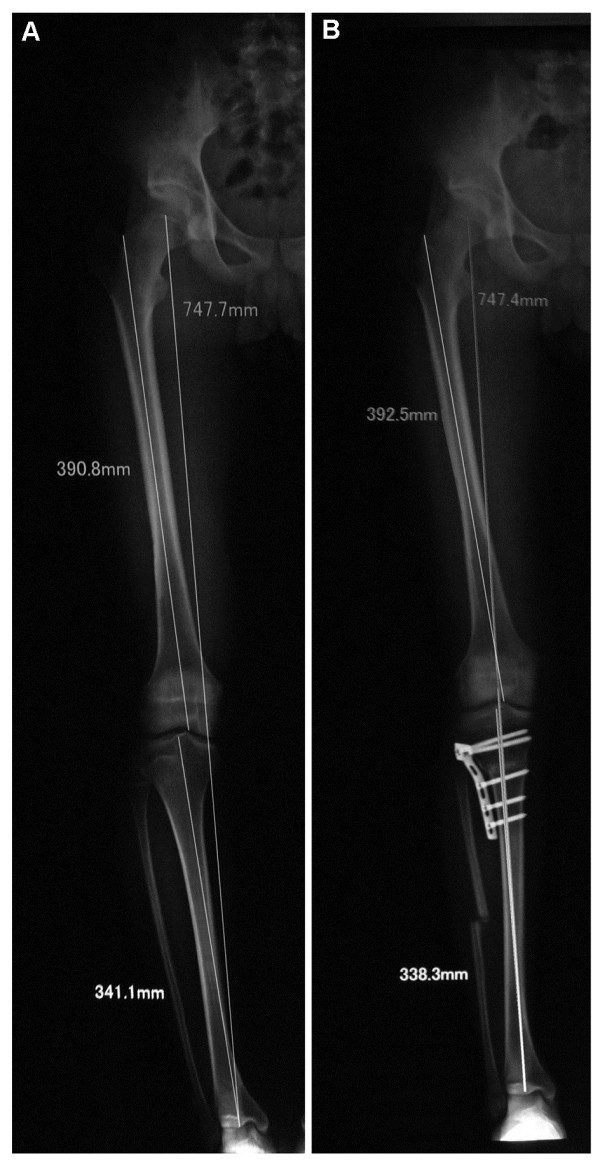
Methods: In this prospective study, young adults with tibia vara and mild medial arthritic changes were included. A CWHTO was performed at the distal third of the tibial tuberosity, instead of the conventional proximal site. An L-shaped locking compression plate was used for internal fixation. Before/after evaluation of femoro-tibial angle (FTA), pain relief, patellar height, and posterior tibial slope were evaluated. Adverse events were monitored.
Results: Seventy-five knees from 46 patients aged 27.2 ± 5.8 years (range, 14-43 years) underwent the modified CWHTO procedure. After a follow-up of 26.3 ± 7.4 months (range, 15-46 months), FTA correction was 12.4° ± 4.7° (range, 7°-31°), and pain was relieved. Reduction in the posterior tibial slope was 3.0° ± 2.3° (p<0.001), while there was no significant change in patella height. Bone union was observed in all patients. There were a delayed union in four knees, a peroneal nerve lesion in five knees causing partial paralysis and/or sensory loss, and infections in two knees. Three patients underwent a second surgery. All adverse events were successfully treated except for a case of extensor hallucis longus muscle paralysis.
Conclusions: The modified CWHTO procedure is efficient and safe for the correction of tibia vara in young patients.
Figures
References
-
- McKellop HA, Llinas A, Sarmiento A. Effects of tibial malalignment on the knee and ankle. Orthop Clin North Am. 1994;25:415–423. - PubMed
-
- Jackson JP, Waugh W. Tibial osteotomy for osteoarthritis of the knee. J Bone Joint Surg Br. 1961;43-B:746–751. - PubMed
-
- Jackson JP, Waugh W. The technique and complications of upper tibial osteotomy. A review of 226 operations. J Bone Joint Surg Br. 1974;56:236–245. - PubMed
-
- Coventry MB. Osteotomy of the upper portion of the tibia for degenerative arthritis of the knee. A preliminary report. J Bone Joint Surg Am. 1965;47:984–990. - PubMed
-
- Moreland JR, Bassett LW, Hanker GJ. Radiographic analysis of the axial alignment of the lower extremity. J Bone Joint Surg Am. 1987;69:745–749. - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
