

Variation in decisions to forgo life-sustaining therapies in US ICUs
- PMID: 24522751
- PMCID: PMC4151359
- DOI: 10.1378/chest.13-2529
Variation in decisions to forgo life-sustaining therapies in US ICUs
Abstract
Background: The magnitude and implication of variation in end-of-life decision-making among ICUs in the United States is unknown.
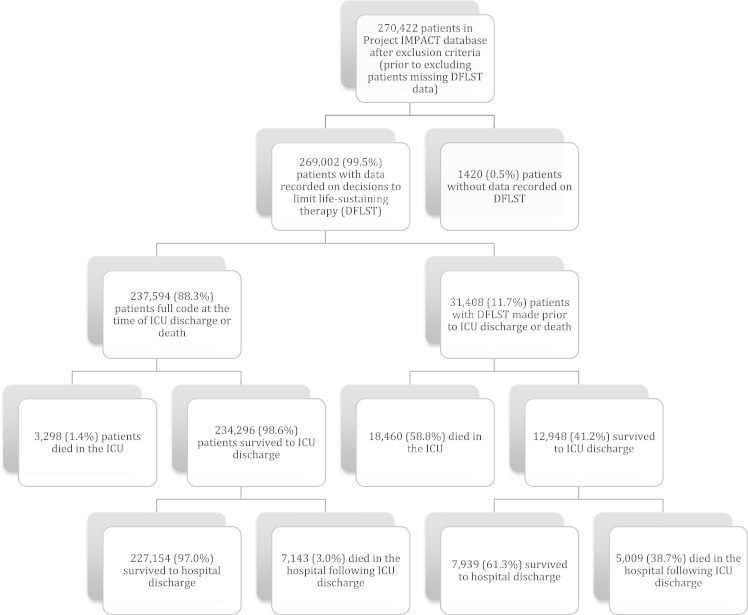
Methods: We reviewed data on decisions to forgo life-sustaining therapy (DFLSTs) in 269,002 patients admitted to 153 ICUs in the United States between 2001 and 2009. We used fixed-effects logistic regression to create a multivariable model for DFLST and then calculated adjusted rates of DFLST for each ICU.
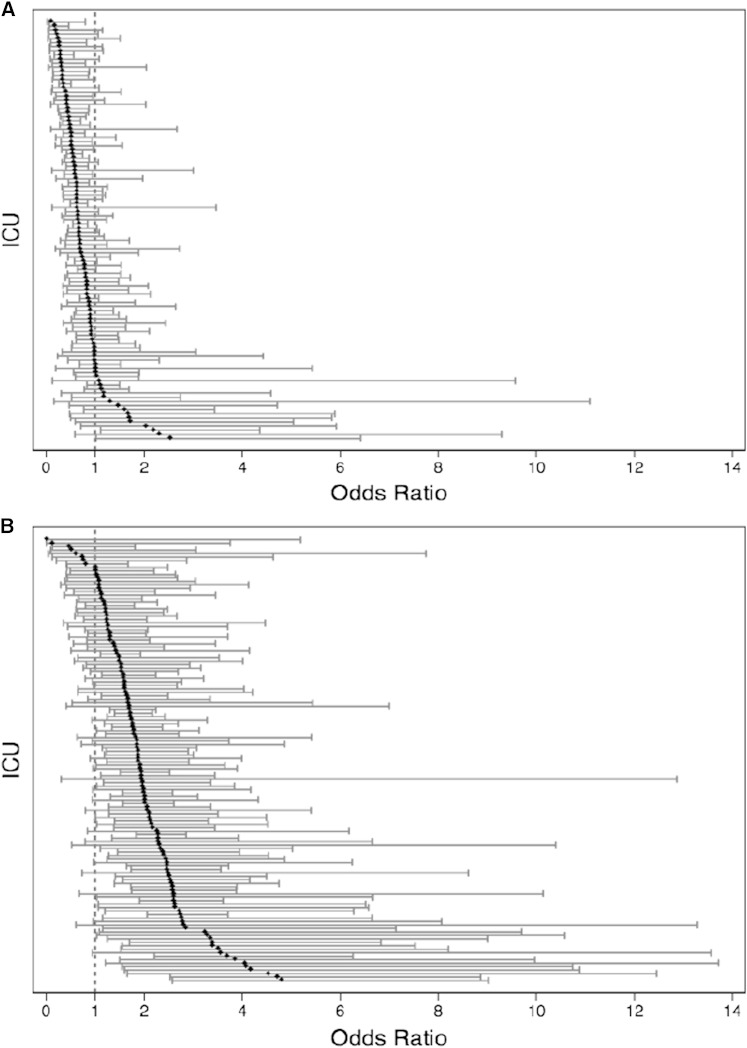
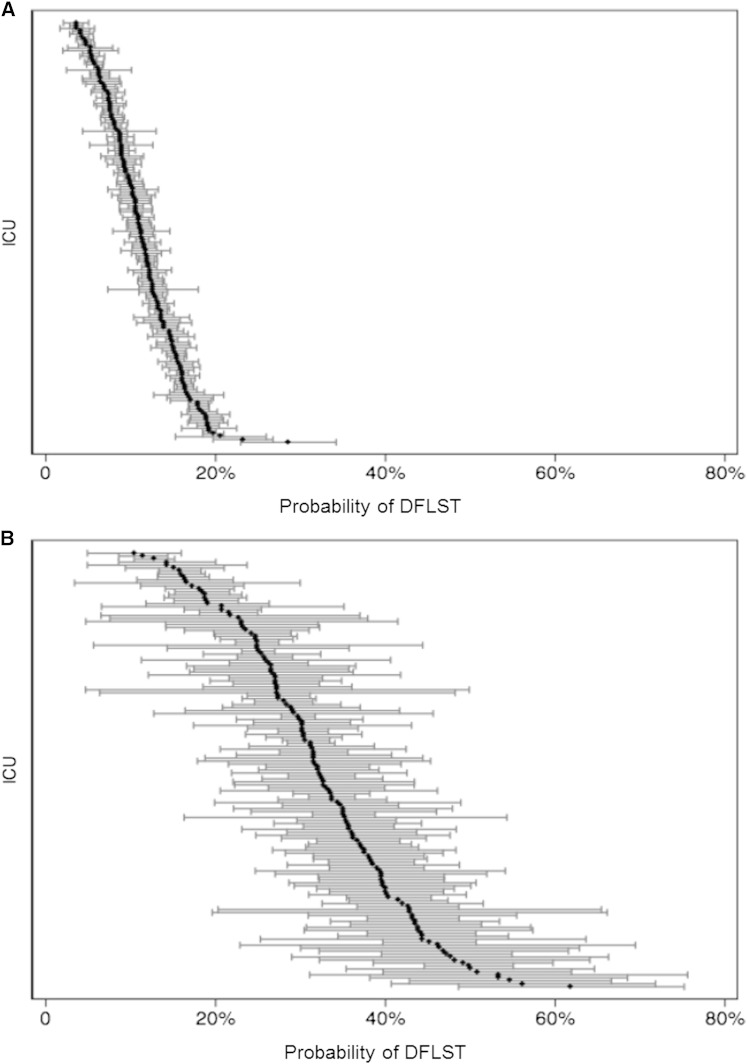
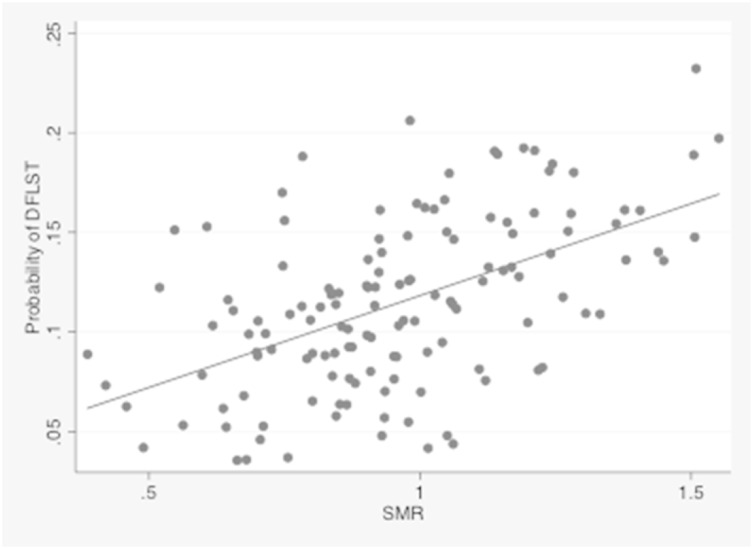
Results: Patient factors associated with increased odds of DFLST included advanced age, female sex, white race, and poor baseline functional status (all P < .001). However, associations with several of these factors varied among ICUs (eg, black race had an OR for DFLST from 0.18 to 2.55 across ICUs). The ICU staffing model was also found to be associated with DFLST, with an open ICU staffing model associated with an increased odds of a DFLST (OR = 1.19). The predicted probability of DFLST varied approximately sixfold among ICUs after adjustment for the fixed patient and ICU effects and was directly correlated with the standardized mortality ratios of ICUs (r = 0.53, 0.41-0.68).
Conclusion: Although patient factors explain much of the variability in DFLST practices, significant effects of ICU culture and practice influence end-of-life decision-making. The observation that an ICU's risk-adjusted propensity to withdraw life support is directly associated with its standardized mortality ratio suggests problems with using the latter as a quality measure.
Figures
Comment in
-
Variability in decisions to limit life-sustaining treatments: is it all about the physician?Chest. 2014 Sep;146(3):532-534. doi: 10.1378/chest.14-0636. Chest. 2014. PMID: 25180716 No abstract available.
-
Palliative vasoactive therapy in patients with septic shock.Chest. 2014 Sep;146(3):e107-e108. doi: 10.1378/chest.14-0602. Chest. 2014. PMID: 25180735 No abstract available.
References
-
- Angus DC, Barnato AE, Linde-Zwirble WT, et al. ; Robert Wood Johnson Foundation ICU End-Of-Life Peer Group. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med. 2004;32(3):638-643. - PubMed
-
- Prendergast TJ, Claessens MT, Luce JM. A national survey of end-of-life care for critically ill patients. Am J Respir Crit Care Med. 1998;158(4):1163-1167. - PubMed
-
- Pochard F, Azoulay E, Chevret S, et al. ; French PROTOCETIC Group. French intensivists do not apply American recommendations regarding decisions to forgo life-sustaining therapy. Crit Care Med. 2001;29(10):1887-1892. - PubMed
-
- Davidson JE, Powers K, Hedayat KM, et al. ; American College of Critical Care Medicine Task Force 2004-2005, Society of Critical Care Medicine. Clinical practice guidelines for support of the family in the patient-centered intensive care unit: American College of Critical Care Medicine Task Force 2004-2005. Crit Care Med. 2007;35(2):605-622. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
