

Variation in do-not-resuscitate orders for patients with ischemic stroke: implications for national hospital comparisons
- PMID: 24523035
- PMCID: PMC3943476
- DOI: 10.1161/STROKEAHA.113.004573
Variation in do-not-resuscitate orders for patients with ischemic stroke: implications for national hospital comparisons
Abstract
Background and purpose: Decisions on life-sustaining treatments and the use of do-not-resuscitate (DNR) orders can affect early mortality after stroke. We investigated the variation in early DNR use after stroke among hospitals in California and the effect of this variation on mortality-based hospital classifications.
Methods: Using the California State Inpatient Database from 2005 to 2011, ischemic stroke admissions for patients aged≥50 years were identified. Cases were categorized by the presence or the absence of DNR orders within the first 24 hours of admission. Multilevel logistic regression models with a random hospital intercept were used to predict inpatient mortality after adjusting for comorbidities, vascular risk factors, and demographics. Hospital mortality rank order was assigned based on this model and compared with the results of a second model that included DNR status.
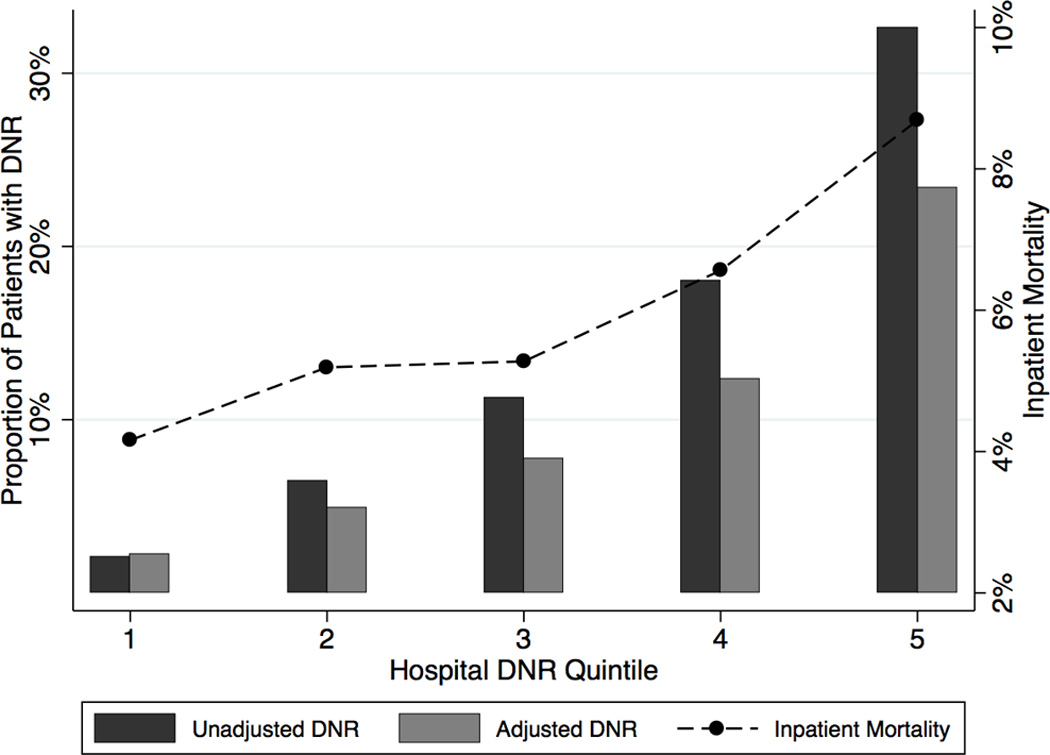
Results: From 355 hospitals, 252,368 cases were identified, including 33,672 (13.3%) with early DNR. Hospital-level-adjusted use of DNR varied widely (quintile 1, 2.2% versus quintile 5, 23.2%). Hospitals with higher early DNR use had higher inpatient mortality because inpatient mortality more than doubled from quintile 1 (4.2%) to quintile 5 (8.7%). Failure to adjust for DNR orders resulted in substantial hospital reclassification across the rank spectrum, including among high mortality hospitals.
Conclusions: There is wide variation in the hospital-level proportion of ischemic stroke patients with early DNR orders; this variation affects hospital mortality estimates. Unless the circumstances of early DNR orders are better understood, mortality-based hospital comparisons may not reliably identify hospitals providing a lower quality of care.
Keywords: mortality; outcome assessment (health care); resuscitation orders; stroke.
Conflict of interest statement
The authors report no conflicts of interest.
Figures

References
-
- Jaren O, Selwa L. Causes of mortality on a university hospital neurology service. Neurologist. 2006;12:245–248. - PubMed
-
- Shepardson LB, Justice AC, Harper DL, Rosenthal GE. Associations between the use of do-not-resuscitate orders and length of stay in patients with stroke. Med Care. 1998;36:AS57–AS67. - PubMed
-
- Shepardson LB, Youngner SJ, Speroff T, O'Brien RG, Smyth KA, Rosenthal GE. Variation in the use of do-not-resuscitate orders in patients with stroke. Arch Intern Med. 1997;157:1841–1847. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
