

Assessment of pancreatic β-cell function: review of methods and clinical applications
- PMID: 24524730
- PMCID: PMC3982570
- DOI: 10.2174/1573399810666140214093600
Assessment of pancreatic β-cell function: review of methods and clinical applications
Abstract
Type 2 diabetes mellitus (T2DM) is characterized by a progressive failure of pancreatic β-cell function (BCF) with insulin resistance. Once insulin over-secretion can no longer compensate for the degree of insulin resistance, hyperglycemia becomes clinically significant and deterioration of residual β-cell reserve accelerates. This pathophysiology has important therapeutic implications. Ideally, therapy should address the underlying pathology and should be started early along the spectrum of decreasing glucose tolerance in order to prevent or slow β-cell failure and reverse insulin resistance. The development of an optimal treatment strategy for each patient requires accurate diagnostic tools for evaluating the underlying state of glucose tolerance. This review focuses on the most widely used methods for measuring BCF within the context of insulin resistance and includes examples of their use in prediabetes and T2DM, with an emphasis on the most recent therapeutic options (dipeptidyl peptidase-4 inhibitors and glucagon-like peptide-1 receptor agonists). Methods of BCF measurement include the homeostasis model assessment (HOMA); oral glucose tolerance tests, intravenous glucose tolerance tests (IVGTT), and meal tolerance tests; and the hyperglycemic clamp procedure. To provide a meaningful evaluation of BCF, it is necessary to interpret all observations within the context of insulin resistance. Therefore, this review also discusses methods utilized to quantitate insulin-dependent glucose metabolism, such as the IVGTT and the euglycemic-hyperinsulinemic clamp procedures. In addition, an example is presented of a mathematical modeling approach that can use data from BCF measurements to develop a better understanding of BCF behavior and the overall status of glucose tolerance.
Figures
References
-
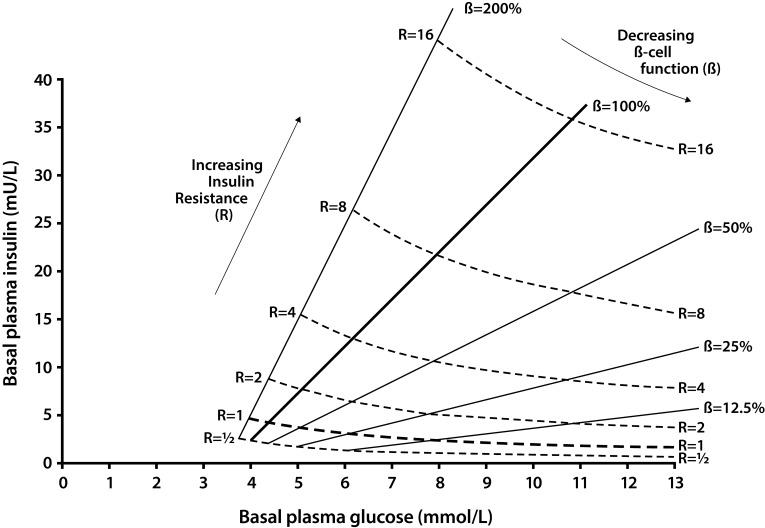
- Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RL. Homeostasis model assessment: insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28:412–9. - PubMed
-
- UK Prospective Diabetes Study Group. UK Prospective Diabetes Study (UKPDS) VIII. Study design, progress and performance. Diabetologia. 1991;34:877–90. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical