

The role of stem cells in osteoarthritis: An experimental study in rabbits
- PMID: 24526748
- PMCID: PMC3926293
- DOI: 10.1302/2046-3758.32.2000187
The role of stem cells in osteoarthritis: An experimental study in rabbits
Abstract
Introduction: Osteoarthritis (OA) is a progressively debilitating disease that affects mostly cartilage, with associated changes in the bone. The increasing incidence of OA and an ageing population, coupled with insufficient therapeutic choices, has led to focus on the potential of stem cells as a novel strategy for cartilage repair.
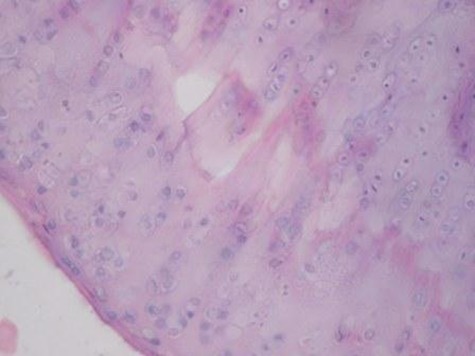
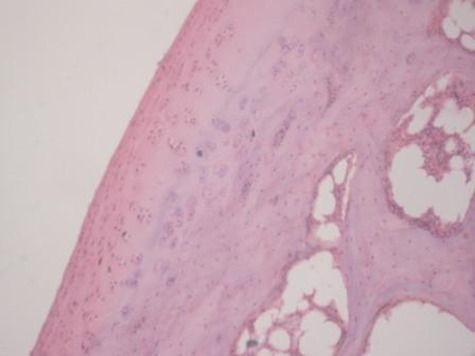
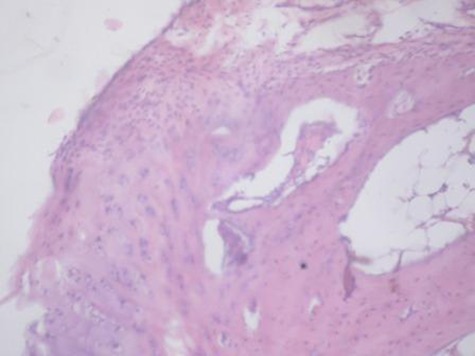
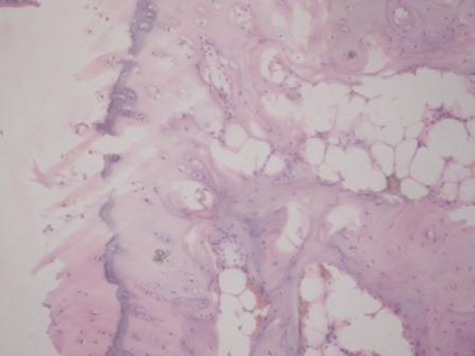
Methods: In this study, we used scaffold-free mesenchymal stem cells (MSCs) obtained from bone marrow in an experimental animal model of OA by direct intra-articular injection. MSCs were isolated from 2.8 kg white New Zealand rabbits. There were ten in the study group and ten in the control group. OA was induced by unilateral transection of the anterior cruciate ligament of the knee joint. At 12 weeks post-operatively, a single dose of 1 million cells suspended in 1 ml of medium was delivered to the injured knee by direct intra-articular injection. The control group received 1 ml of medium without cells. The knees were examined at 16 and 20 weeks following surgery. Repair was investigated radiologically, grossly and histologically using haematoxylin and eosin, Safranin-O and toluidine blue staining.
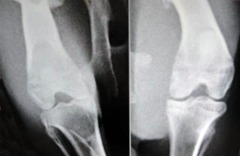
Results: Radiological assessment confirmed development of OA changes after 12 weeks. Rabbits receiving MSCs showed a lower degree of cartilage degeneration, osteophyte formation, and subchondral sclerosis than the control group at 20 weeks post-operatively. The quality of cartilage was significantly better in the cell-treated group compared with the control group after 20 weeks.
Conclusions: Bone marrow-derived MSCs could be promising cell sources for the treatment of OA. Neither stem cell culture nor scaffolds are absolutely necessary for a favourable outcome. Cite this article: Bone Joint Res 2014;3:32-7.
Keywords: MSC; Mesenchymal stem cells; OA; Osteoarthritis; Rabbit model; Repair.
Conflict of interest statement
Figures





References
-
- Brooks PM. Impact of osteoarthritis on individuals and society: how much disability?: social consequences and health economic implications. Curr Opin Rheumatol 2002;14:573–577 - PubMed
-
- Dennison E, Cooper C. Osteoarthritis: epidemiology and classification. In: Hochberg MC, Silman AJ, Smolen JS, et al, eds. Rheumatology London: Mosby, 2003:1781–1791.
-
- Lapsley HM, March LM, Tribe KL, Cross MJ, Brooks PM. Living with osteoarthritis: patient expenditures, health status, and social impact. Arthritis Rheum 2001;45:301–306 - PubMed
-
- Mapel DW, Shainline M, Paez K, Gunter M. Hospital, pharmacy, and outpatient costs for osteoarthritis and chronic back pain. J Rheumatol 2004;31:573–583 - PubMed
-
- Brandt KD, Dieppe P, Radin EL. Etiopathogenesis of osteoarthritis. Rheum Dis Clin North Am 2008;34:531–559 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
