

Venous ulcers: new options in treatment: minimally invasive vein surgery
- PMID: 24527103
- PMCID: PMC3478919
- DOI: 10.1016/j.jcws.2008.10.004
Venous ulcers: new options in treatment: minimally invasive vein surgery
Abstract
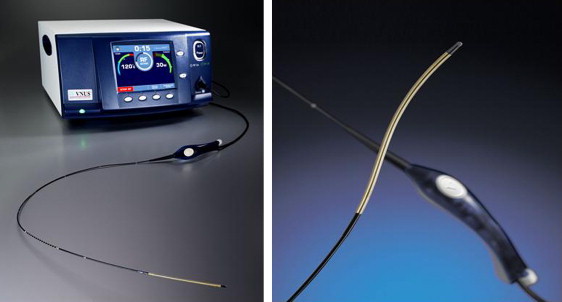
Venous disease has a spectrum of presentations. The most advanced state of chronic venous insufficiency (CVI) managed by wound care specialists being ulceration of the lower extremity. The goal of all treatments for advanced venous disease is to decrease ambulatory venous hypertension. Treatment can be divided into exogenous and endogenous methods. Exogenous methods include those applied externally such as compression, elevation, debridement and wound dressings. Endogenous methods treat the underlying venous pathology either due to venous valvular dysfunction or venous obstruction leading to venous hypertension. Recently, significant advances in endogenous methods have evolved. The development of a new concept, minimally invasive vein surgery (MIVS), has improved upon traditional, open, invasive treatments of venous disease. MIVS techniques are performed percutaneously, with minimal anesthesia, no incisions and rarely require hospital admission. This article summarizes the concept of MIVS, describes each method of MIVS and its complementary role in the management of venous leg ulcers patients.
Keywords: MIVS; PAPs; SEPS; laser ablation; minimally invasive vein surgery; perforator ablation; radiofrequency ablation; venous ulcer.
Figures

Similar articles
-
Minimally invasive vein surgery: latest options for vein disease.Mt Sinai J Med. 2010 May-Jun;77(3):270-8. doi: 10.1002/msj.20186. Mt Sinai J Med. 2010. PMID: 20506452 Review.
-
The management of chronic venous insufficiency with ulceration: the role of minimally invasive perforator interruption.Ann Vasc Surg. 2013 Jan;27(1):89-95. doi: 10.1016/j.avsg.2012.09.001. Ann Vasc Surg. 2013. PMID: 23257074
-
Minimally invasive vein surgery: its role in the treatment of venous stasis ulceration.Am J Surg. 2004 Jul;188(1A Suppl):26-30. doi: 10.1016/S0002-9610(03)00288-5. Am J Surg. 2004. PMID: 15223499 Review.
-
Endovascular radiofrequency ablation for varicose veins: an evidence-based analysis.Ont Health Technol Assess Ser. 2011;11(1):1-93. Epub 2011 Feb 1. Ont Health Technol Assess Ser. 2011. PMID: 23074413 Free PMC article.
-
Iliac-femoral venous stenting for lower extremity venous stasis symptoms.Ann Vasc Surg. 2012 Feb;26(2):185-9. doi: 10.1016/j.avsg.2011.05.033. Epub 2011 Oct 22. Ann Vasc Surg. 2012. PMID: 22018502
Cited by
-
Protocol for a systematic review and meta-analysis of interventions for pathologic perforator veins in chronic venous disease.BMJ Open. 2019 May 1;9(4):e024088. doi: 10.1136/bmjopen-2018-024088. BMJ Open. 2019. PMID: 31048426 Free PMC article.
References
-
- Adams F., editor. The Genuine Works of Hippocrates. Sydenham Society; London, England: 1849. Hippocrates: De ulceribus and de carnibus; pp. 325–336.
-
- Beebe H.G., Bergan J.J., Bergqvist D. Classification and grading of chronic venous disease in the lower limbs: A consensus statement. Eur J Vasc Endovasc Surg. 1996;12(4):487–491. - PubMed
-
- Eklof B., Rutherford R.B., Bergan J.J. Revision of the CEAP classification for chronic venous disorders: Consensus statement. J Vasc Surg. 2004;40(6):1248–1252. - PubMed
LinkOut - more resources
Full Text Sources
