

Intraductal endoscopic radiofrequency ablation for the treatment of hilar non-resectable malignant bile duct obstruction
- PMID: 24527176
- PMCID: PMC3921441
- DOI: 10.4253/wjge.v6.i1.13
Intraductal endoscopic radiofrequency ablation for the treatment of hilar non-resectable malignant bile duct obstruction
Abstract
Aim: To evaluate the safety and technical success of endoscopic radiofrequency ablation (RFA) for palliative treatment of malignant hilar bile duct obstruction.
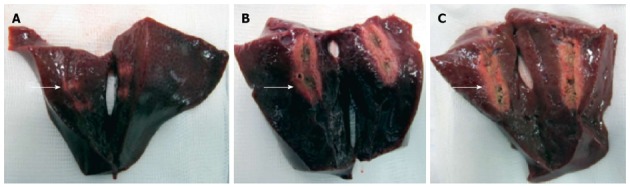
Methods: In this study, a recently CE and FDA-approved endoscopic RFA catheter was first tested in an ex vivo pig liver model to study the effect of electrosurgical variables on the extent of the area of induced necrosis. Subsequently, a retrospective analysis was conducted of all patients treated with endoscopic RFA for malignant biliary obstruction at our center between February 2012 and April 2013. All patients received an additional plastic stent implantation into the biliary tree following RFA.
Results: In the pig model, ablation time of 60-90 seconds using the bipolar soft coagulation mode at 8-10 watts with an effect of 8 was found to be the most feasible setting. Twelve patients (5 females, 7 males; mean age, 70 years) underwent 19 endoscopic RFA (range, 1-5) sessions. Deployment of RFA was successful in all patients. Systemic chemotherapy was administered in four patients. We observed biliary bleeding 4-6 wk after the intervention in three cases and two of these patients died: in one patient, spontaneous hemobilia occurred, whereas bleeding started during stent extraction in the other. In the third patient, bleeding was stopped by insertion of a non-covered self-expanding metal stent. Another three patients developed cholangitis during follow-up. Seven patients died during follow-up and median survival was 6.4 mo (95%CI: 0.05-12.7) from the time of the first RFA.
Conclusion: Endoscopic RFA is an easy to perform and technically highly successful procedure. However, hemobilia possibly associated with RFA occurred in three of our patients. Therefore, larger prospective studies are needed to further evaluate the safety and efficacy of this promising new method.
Keywords: Bile duct cancer; Cholangiocarcinoma; Cholangiography; Endoscopic retrograde cholangiopancreatography; Endoscopy; Radiofrequency ablation.
Figures




References
-
- Valle J, Wasan H, Palmer DH, Cunningham D, Anthoney A, Maraveyas A, Madhusudan S, Iveson T, Hughes S, Pereira SP, et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N Engl J Med. 2010;362:1273–1281. - PubMed
-
- Demols A, Maréchal R, Devière J, Van Laethem JL. The multidisciplinary management of gastrointestinal cancer. Biliary tract cancers: from pathogenesis to endoscopic treatment. Best Pract Res Clin Gastroenterol. 2007;21:1015–1029 Available]. - PubMed
-
- Ortner ME, Caca K, Berr F, Liebetruth J, Mansmann U, Huster D, Voderholzer W, Schachschal G, Mössner J, Lochs H. Successful photodynamic therapy for nonresectable cholangiocarcinoma: a randomized prospective study. Gastroenterology. 2003;125:1355–1363. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
