

Clinically Addressing Biofilm in Chronic Wounds
- PMID: 24527292
- PMCID: PMC3839004
- DOI: 10.1089/wound.2011.0333
Clinically Addressing Biofilm in Chronic Wounds
Abstract
Background: A chronic wound is a wound that is arrested in the inflammatory phase of wound healing and cannot progress further. Over 90% of chronic wounds contain bacteria and fungi living within a biofilm construct.
The problem: Each aggregation of microbes creates a distinct biofilm with differing characteristics so that a clinical approach has to be tailored to the specifics of a given biofilm. Defining the characteristics of that biofilm and then designing a therapeutic option particular to that biofilm is currently being defined.
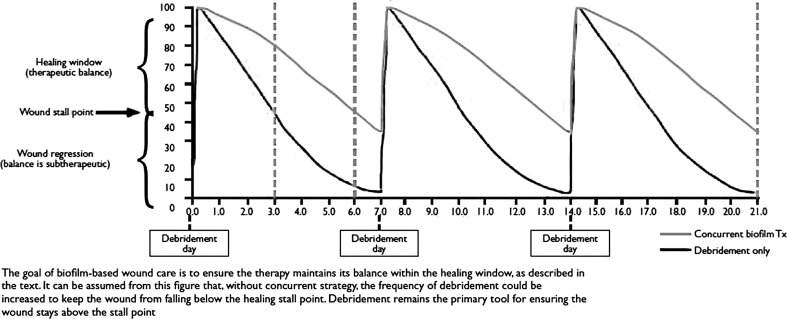
Basic/clinical science advances: Biofilm becomes resistant to therapeutic maneuvers at 48-96 h after formation. By repeatedly attacking it on a regular schedule, one forces biofilm to reattach and reform during which time it is susceptible to antibiotics and host defenses. Identifying the multiple bacteria and fungi that make up a specific biofilm using polymerase chain reaction (PCR) allows directed therapeutic maneuvers such as application of specific topical antibiotics and biocides to increase the effectiveness of the debridement.
Clinical care relevance: Most chronic wounds contain biofilm that perpetuate the inflammatory phase of wound healing. Combining debridement with using PCR to identify the bacteria and fungi within the biofilm allows for more targeted therapeutic maneuvers to eliminate a given biofilm.
Conclusion: Therapeutic options in addition to debridement are currently being evaluated to address biofilm. Using PCR to direct adjunctive therapeutic maneuvers may increase the effectiveness of addressing biofilm in a chronic wound.
Figures

References
-
- Cornell RS. Meyr AJ. Steinberg JS. Attinger CE. Debridement of the noninfected wound. J Vasc Surg. 2010;52:31S. - PubMed
-
- Clark RA. Oxidative stress and “senescent” fibroblasts in non-healing wounds as potential therapeutic targets. J Invest Dermatol. 2008;128:2361. - PubMed
-
- Cho KH. Caparon MG. Patterns of virulence gene expression differ between biofilm and tissue communities of Streptococcus pyogenes. Mol Microbiol. 2005;57:6–1545. - PubMed
-
- Steed DL. Donohoe D. Webster MW. Lindsley L. Effect of extensive debridement and treatment on the healing of diabetic foot ulcers. Diabetic Ulcer Study Group. J Am Coll Surg. 1996;183:61. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
