

Electrical Stimulation Therapy and Wound Healing: Where Are We Now?
- PMID: 24527312
- PMCID: PMC3839020
- DOI: 10.1089/wound.2011.0351
Electrical Stimulation Therapy and Wound Healing: Where Are We Now?
Abstract
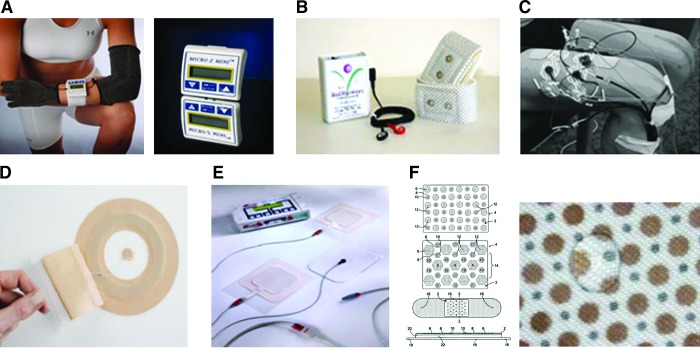
Background: Healing chronic wounds is an ongoing challenge for clinicians and poses a serious public health burden. Electrical stimulation (ES), broadly defined as the application of electrical current via electrodes placed on the skin adjacent to or directly within the wound, has been proposed as a therapeutic modality over a century ago, and recent advances in understanding the biology of electrical phenomena in the skin have rekindled an interest in this modality.
The problem: Despite evidence that has shown ES to be effective for wound healing, it has been slow to gain acceptance in the United States. Also, there has been no consensus in terms of standardization of parameters to devise a systematic protocol for implementation of this technology.
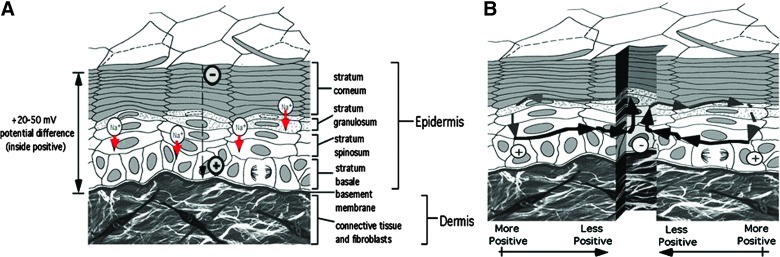
Basic/clinical science advances: The epidermis maintains a "skin battery" that generates an endogenous electric field and current flow when wounded. Experimental models have demonstrated that most of the cell types within the wound can sense an electric field in the range of that endogenously generated in the wound, and respond with a variety of biological and functional responses that can contribute to healing. Multiple animal wound models have demonstrated enhancement of a number of parameters of healing when ES is exogenously supplied.
Clinical care relevance: Clinical trials have investigated the efficacy of multiple forms of ES for improving healing in a wide variety of human chronic wounds. In 2002 the Centers for Medicare and Medicaid Services approved reimbursement for use of ES in a clinical setting for certain chronic wounds.
Conclusion: THERE REMAIN MANY VOIDS IN OUR KNOWLEDGE BASE: clinical evidence is limited by deficiencies in the design of many of the trials, a multiplicity of ES application modes and waveforms used in trials prevent selection of an optimal modality, and lack of uniformity in reporting ES dosages leave us not much advanced from our clinical knowledge base a decade ago.
Figures

Similar articles
-
Electrical Stimulation of Wound Healing: A Review of Animal Experimental Evidence.Adv Wound Care (New Rochelle). 2014 Feb 1;3(2):202-218. doi: 10.1089/wound.2012.0409. Adv Wound Care (New Rochelle). 2014. PMID: 24761359 Free PMC article. Review.
-
The efficacy of electrical stimulation in experimentally induced cutaneous wounds in animals.Vet Dermatol. 2016 Aug;27(4):235-e57. doi: 10.1111/vde.12328. Epub 2016 May 18. Vet Dermatol. 2016. PMID: 27189048 Review.
-
The combined effect of a three-channel electrode delivery system with local heat on the healing of chronic wounds.Diabetes Technol Ther. 2009 Oct;11(10):681-8. doi: 10.1089/dia.2009.0024. Diabetes Technol Ther. 2009. PMID: 19821762
-
Electrical Stimulation to Enhance Wound Healing.J Funct Biomater. 2021 Jun 19;12(2):40. doi: 10.3390/jfb12020040. J Funct Biomater. 2021. PMID: 34205317 Free PMC article. Review.
-
Electrical Stimulation and Cutaneous Wound Healing: A Review of Clinical Evidence.Healthcare (Basel). 2014 Oct 27;2(4):445-67. doi: 10.3390/healthcare2040445. Healthcare (Basel). 2014. PMID: 27429287 Free PMC article. Review.
Cited by
-
A systematic review of electrical stimulation for pressure ulcer prevention and treatment in people with spinal cord injuries.J Spinal Cord Med. 2014 Nov;37(6):703-18. doi: 10.1179/2045772314Y.0000000226. Epub 2014 Jun 26. J Spinal Cord Med. 2014. PMID: 24969965 Free PMC article.
-
Physicochemically Tuned Myofibroblasts for Wound Healing Strategy.Sci Rep. 2019 Nov 5;9(1):16070. doi: 10.1038/s41598-019-52523-9. Sci Rep. 2019. PMID: 31690789 Free PMC article.
-
Microcurrent Stimulation Triggers MAPK Signaling and TGF-β1 Release in Fibroblast and Osteoblast-Like Cell Lines.Cells. 2020 Aug 19;9(9):1924. doi: 10.3390/cells9091924. Cells. 2020. PMID: 32825091 Free PMC article.
-
Come together: On-chip bioelectric wound closure.Biosens Bioelectron. 2021 Nov 15;192:113479. doi: 10.1016/j.bios.2021.113479. Epub 2021 Jul 8. Biosens Bioelectron. 2021. PMID: 34265520 Free PMC article.
-
Applied Electric Fields Polarize Initiation and Growth of Endothelial Sprouts.J Tissue Eng Regen Med. 2023 Dec 23;2023:6331148. doi: 10.1155/2023/6331148. eCollection 2023. J Tissue Eng Regen Med. 2023. PMID: 40226427 Free PMC article.
References
-
- Sheehan P. Jones P. Caselli A. Giurini JM. Veves A. Percent change in wound area of diabetic foot ulcers over a 4-week period is a robust predictor of complete healing in a 12-week prospective trial. Diabetes Care. 2003;26:1879. - PubMed
-
- Snyder RJ. Kirsner RS. Warriner RA., 3rd Lavery LA. Hanft JR. Sheehan P. Consensus recommendations on advancing the standard of care for treating neuropathic foot ulcers in patients with diabetes. Ostomy Wound Manage. 2010;56(4 Suppl):S1. - PubMed
-
- Kloth L. Zhao M. Endogenous, exogenous electrical fields for wound healing. In: McCulloch J, editor; Kloth L, editor. Wound Healing: Evidence-Based Management. 4th. Brick, NJ: F.A. Davis; 2009. pp. 450–513.
-
- Reiber GE. Ledoux WR. Epidemiology of diabetic foot ulcers, amputations: evidence for prevention. In: Williams R, editor; Herman W, editor; Kinmonth AL, editor; Wareham NJ, editor. The Evidence Base for Diabetes Care. Hoboken, NJ: John Wiley & Sons; 2002. pp. 641–665.
-
- Boulton AJ. Vileikyte L. Ragnarson-Tennvall G. Apelqvist J. The global burden of diabetic foot disease. Lancet. 2005;366:1719. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
