

Continuous selective intra-arterial application of nimodipine in refractory cerebral vasospasm due to aneurysmal subarachnoid hemorrhage
- PMID: 24527461
- PMCID: PMC3914346
- DOI: 10.1155/2014/970741
Continuous selective intra-arterial application of nimodipine in refractory cerebral vasospasm due to aneurysmal subarachnoid hemorrhage
Abstract
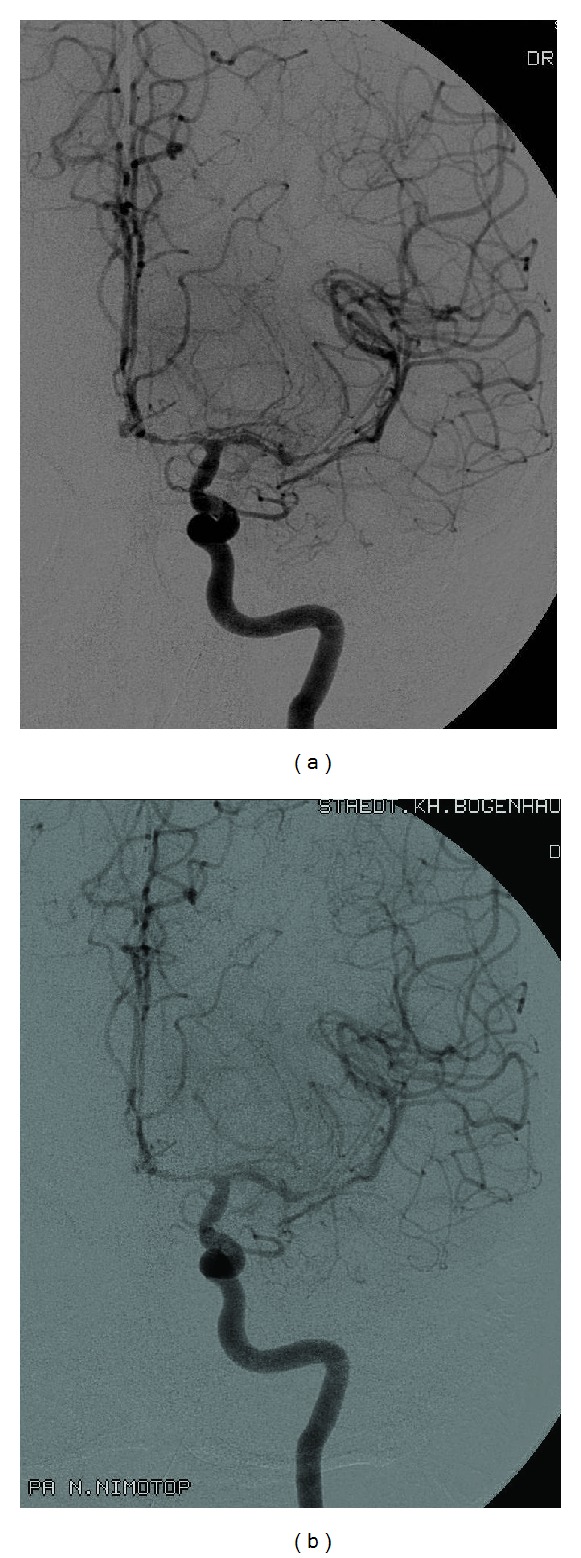
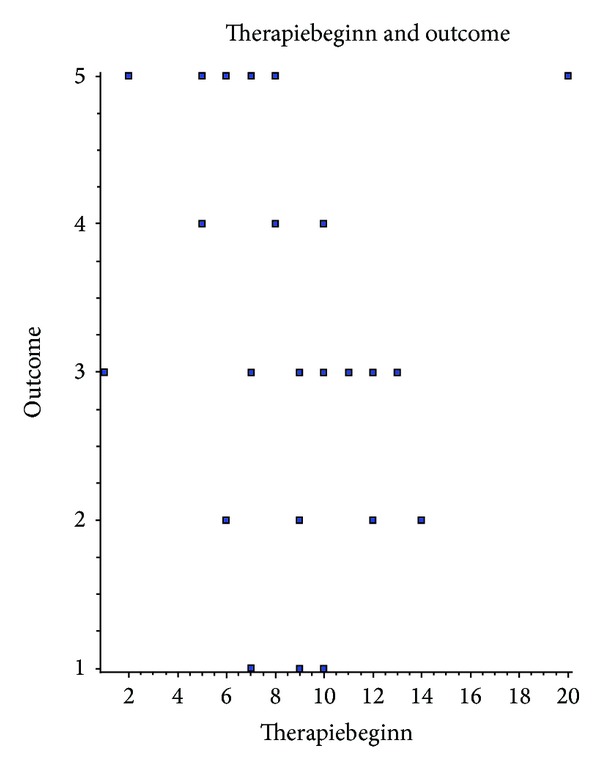
Background: Cerebral vasospasm is one of the leading courses for disability in aneurysmal subarachnoid hemorrhage. Effective treatment of vasospasm is therefore one of the main priorities for these patients. We report about a case series of continuous intra-arterial infusion of the calcium channel antagonist nimodipine for 1-5 days on the intensive care unit.
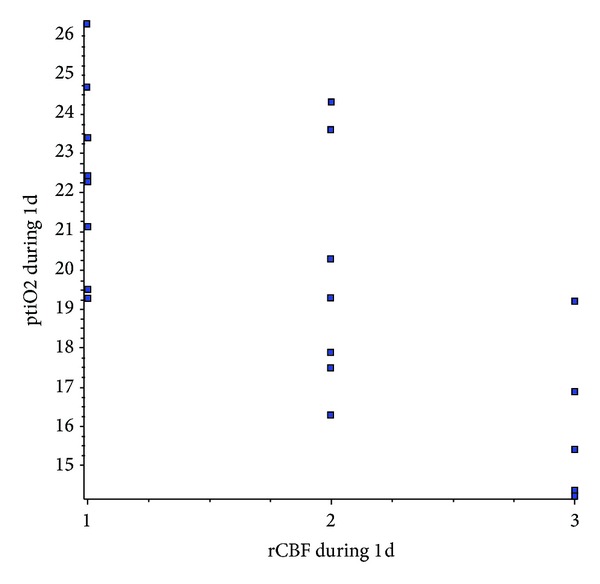
Methods: In thirty patients with aneurysmal subarachnoid hemorrhage and refractory vasospasm continuous infusion of nimodipine was started on the neurosurgical intensive care unit. The effect of nimodipine on brain perfusion, cerebral blood flow, brain tissue oxygenation, and blood flow velocity in cerebral arteries was monitored.
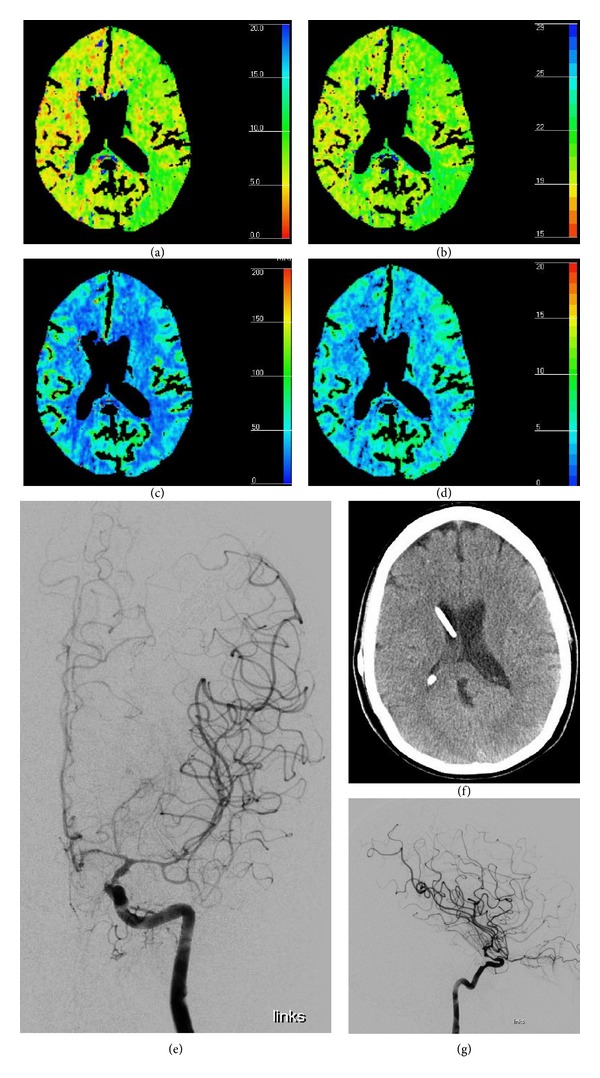
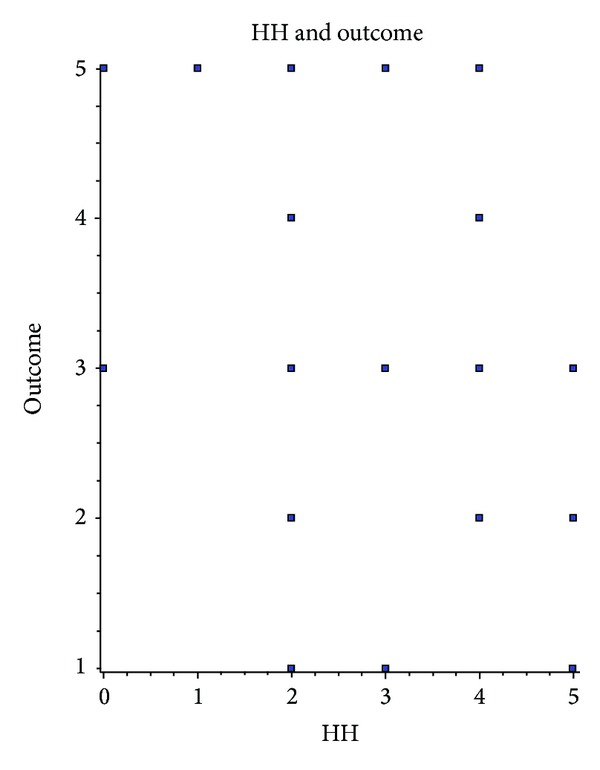
Results: Based on Hunt & Hess grades on admission, 83% survived in a good clinical condition and 23% recovered without an apparent neurological deficit. Persistent ischemic areas were seen in 100% of patients with GOS 1-3 and in 69% of GOS 4-5 patients. Regional cerebral blood flow and computed tomography perfusion scanning showed adequate correlation with nimodipine application and angiographic vasospasm. Transcranial Doppler turned out to be unreliable with interexaminer variance and failure of detecting vasospasm or missing the improvement.
Conclusion: Local continuous intra-arterial nimodipine treatment for refractory cerebral vasospasm after aSAH can be recommended as a low-risk treatment in addition to established endovascular therapies.
Figures
References
-
- Broderick JP, Brott T, Tomsick T, Miller R, Huster G. Intracerebral hemorrhage more than twice as common as subarachnoid hemorrhage. Journal of Neurosurgery. 1993;78(2):188–191. - PubMed
-
- Linn FHH, Rinkel GJE, Algra A, van Gijn J. Incidence of subarachnoid hemorrhage: role of region, year, and rate of computed tomography: a meta-analysis. Stroke. 1996;27(4):625–629. - PubMed
-
- Sarti C, Tuomilehto J, Salomaa V, et al. Epidemiology of subarachnoid hemorrhage in Finland from 1983 to 1985. Stroke. 1991;22(7):848–853. - PubMed
-
- Greenberg MS. Handbook of Neurosurgery. 7th edition. chapter 30. New York, NY, USA: Thieme; 2010. SAH and aneurysms; introduction to SAH; p. p. 1034.
-
- Solenski NJ, Haley EC, Jr., Kassell NF, et al. Medical complications of aneurysmal subarachnoid hemorrhage: a report of the multicenter, cooperative aneurysm study. Critical Care Medicine. 1995;23(6):1007–1017. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
