

Medical treatment of aortic aneurysms in Marfan syndrome and other heritable conditions
- PMID: 24527681
- PMCID: PMC4021286
- DOI: 10.2174/1573403x1002140506124902
Medical treatment of aortic aneurysms in Marfan syndrome and other heritable conditions
Abstract
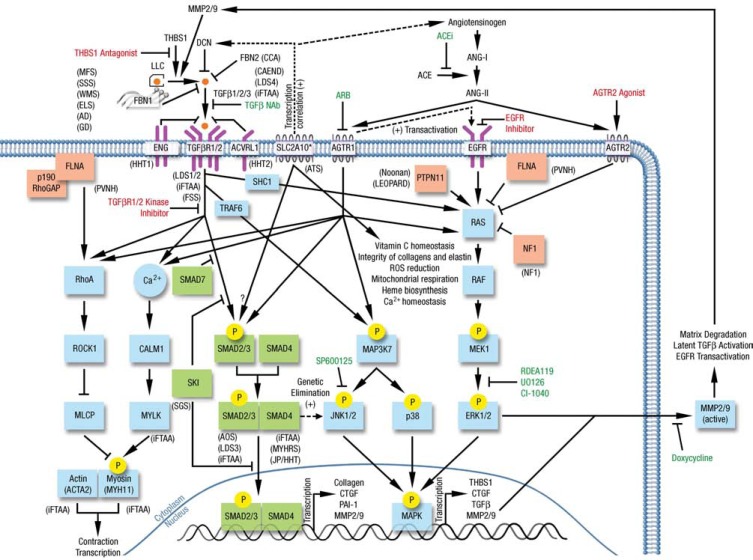
Thoracic aortic aneurysms can be triggered by genetic disorders such as Marfan syndrome (MFS) and related aortic diseases as well as by inflammatory disorders such as giant cell arteritis or atherosclerosis. In all these conditions, cardiovascular risk factors, such as systemic arterial hypertension, may contribute to faster rate of aneurysm progression. Optimal medical management to prevent progressive aortic dilatation and aortic dissection is unknown. β-blockers have been the mainstay of medical treatment for many years despite limited evidence of beneficial effects. Recently, losartan, an angiotensin II type I receptor antagonist (ARB), has shown promising results in a mouse model of MFS and subsequently in humans with MFS and hence is increasingly used. Several ongoing trials comparing losartan to β-blockers and/or placebo will better define the role of ARBs in the near future. In addition, other medications, such as statins and tetracyclines have demonstrated potential benefit in experimental aortic aneurysm studies. Given the advances in our understanding of molecular mechanisms triggering aortic dilatation and dissection, individualized management tailored to the underlying genetic defect may be on the horizon of individualized medicine. We anticipate that ongoing research will address the question whether such genotype/pathogenesis-driven treatments can replace current phenotype/syndrome-driven strategies and whether other forms of aortopathies should be treated similarly. In this work, we review currently used and promising medical treatment options for patients with heritable aortic aneurysmal disorders.
Figures
References
-
- Johnston KW, Rutherford RB, Tilson MD, Shah DM, Hollier L, Stanley JC. Suggested standards for reporting on arterial aneurysms.Subcommittee on Reporting Standards for Arterial Aneursms.ad hoc Committee on Reporting Standards., Society for Vascular Surgery and North American Chapter., International Society for Cardiovascular Surgery. J Vasc Surg . 1991;13(3):452–8. - PubMed
-
- Coady MA, Rizzo JA, Goldstein LJ, Elefteriades JA. Natural history. pathogensis.and etiology of thoracic aortic aneurysms and dissections. Cardiol Clin. 1999; 17:615–35. - PubMed
-
- Ito S, Akutsu K, Tamori Y , et al. Differences in atherosclerotic profiles between patients with thoracic and abdominal aortic aneurysms. Am J Cardiol. 2008;101:696–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
