

Polyarteritis nodosa complicated by posterior reversible encephalopathy syndrome: a case report
- PMID: 24529495
- PMCID: PMC3930290
- DOI: 10.1186/1756-0500-7-89
Polyarteritis nodosa complicated by posterior reversible encephalopathy syndrome: a case report
Abstract
Background: Posterior reversible encephalopathy syndrome is a presentation which is diagnosed clinico-radiologically. The primary aetiological processes leading to posterior reversible encephalopathy syndrome are many, which include autoimmune conditions. Polyarteritis nodosa as an aetiological factor for posterior reversible encephalopathy syndrome is rare. We present a case of polyarteritis nodosa complicated by posterior reversible encephalopathy syndrome.
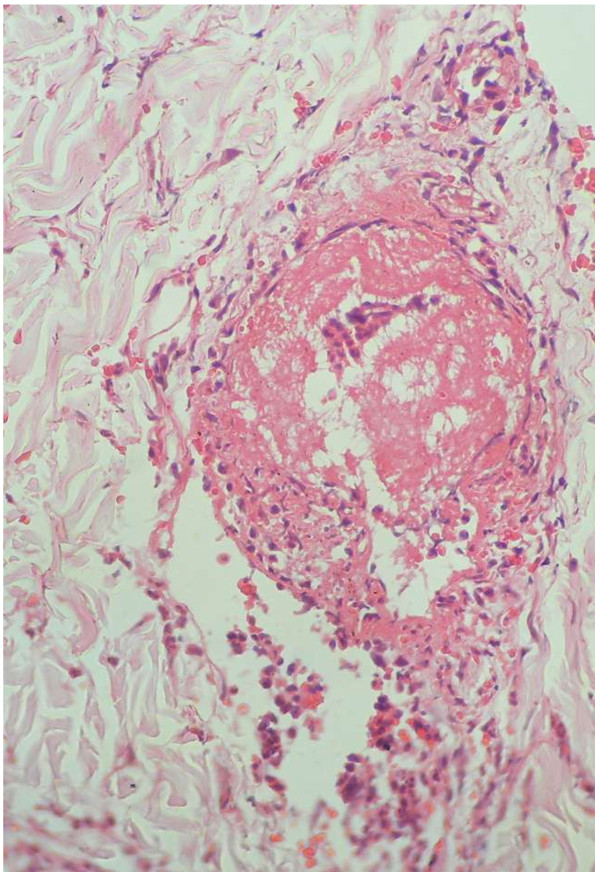
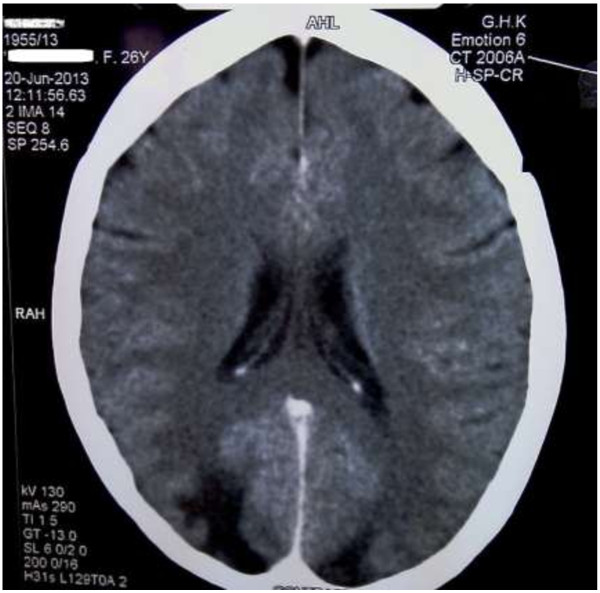
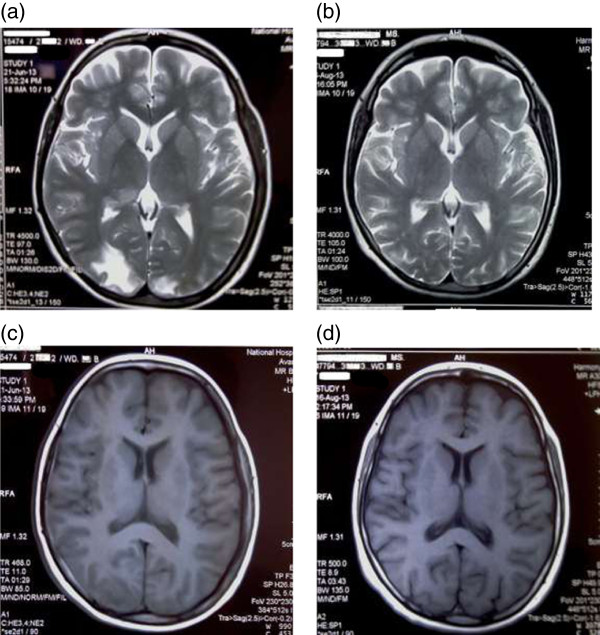
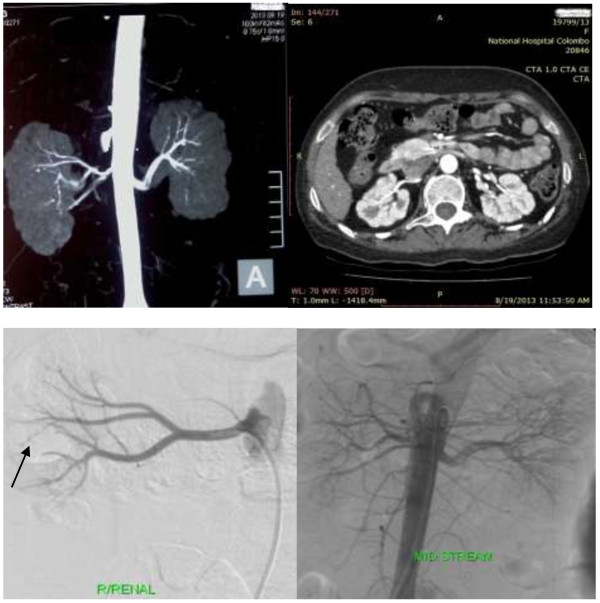
Case presentation: A 26-year-old South-Asian female presented with left sided focal seizures with secondary generalization and visual disturbance for 2 days duration. She had a prior history of arthralgia and weight loss with no medically explainable cause for young onset hypertension. Examination revealed a right claw hand with a palpable vasculitic type of rash involving both the palmar surfaces. Symptoms responded to management with anti-hypertensives and anti-epileptics. Whole blood count, iron studies, erythrocyte sedimentation rate and C-reactive protein values portrayed an ongoing chronic inflammatory process. Serological studies such as Anti-nuclear antibody, Anti -double stranded deoxyribonucleic acid, Anti-neutrophil cytoplasmic antibody and Anti-cyclic citrulinated peptide were negative. Magnetic resonance imaging revealed high signal intensity on T2 in both occipital lobes. Skin biopsy of the palm revealed moderate vessel vasculitis. Renal imaging revealed structurally abnormal kidneys with micro aneurysms in the right renal vasculature. Repeat magnetic resonance imaging of the brain two months later showed marked improvement. A diagnosis of polyarteritis nodosa with posterior reversible encephalopathy syndrome was made.
Conclusions: Posterior reversible encephalopathy syndrome should not be missed. Investigations for an aetio-pathological cause should be considered including the rarer associations like polyarteritis nodosa.
Figures

References
-
- Arai M, Shigeno K, Wada M. A reversible posterior leukoencephalopathy syndrome in a patient with classical polyarteritis nodosa]. Rinsho shinkeigaku. Rinsho Shinkeigaku. 1997;37:64–66. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
