

Preterm birth, infant weight gain, and childhood asthma risk: a meta-analysis of 147,000 European children
- PMID: 24529685
- PMCID: PMC4024198
- DOI: 10.1016/j.jaci.2013.12.1082
Preterm birth, infant weight gain, and childhood asthma risk: a meta-analysis of 147,000 European children
Abstract
Background: Preterm birth, low birth weight, and infant catch-up growth seem associated with an increased risk of respiratory diseases in later life, but individual studies showed conflicting results.
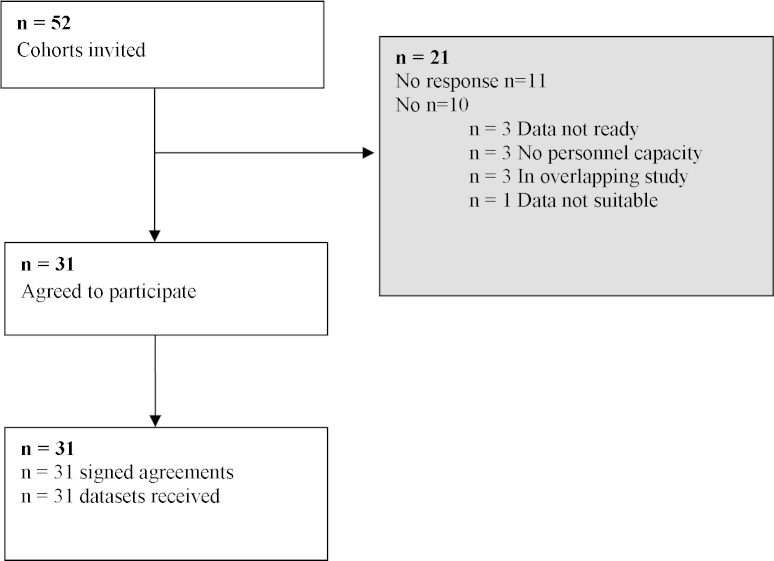
Objectives: We performed an individual participant data meta-analysis for 147,252 children of 31 birth cohort studies to determine the associations of birth and infant growth characteristics with the risks of preschool wheezing (1-4 years) and school-age asthma (5-10 years).
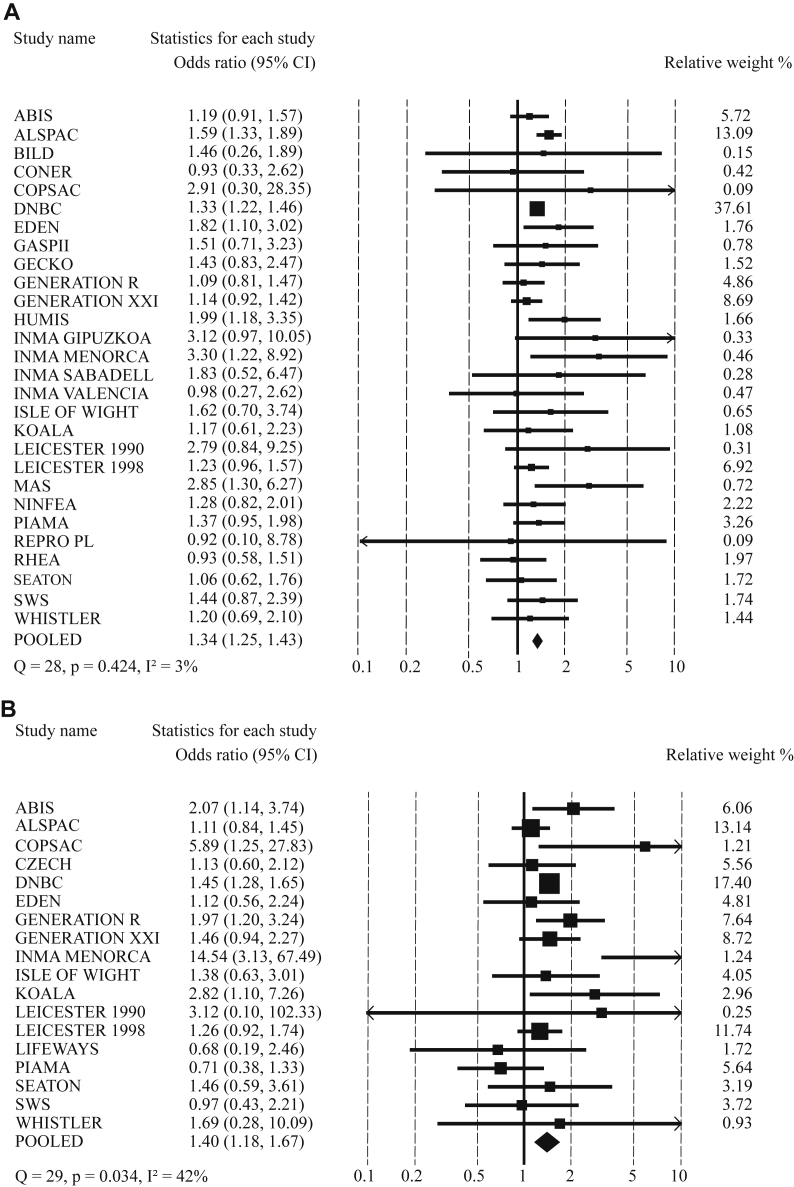
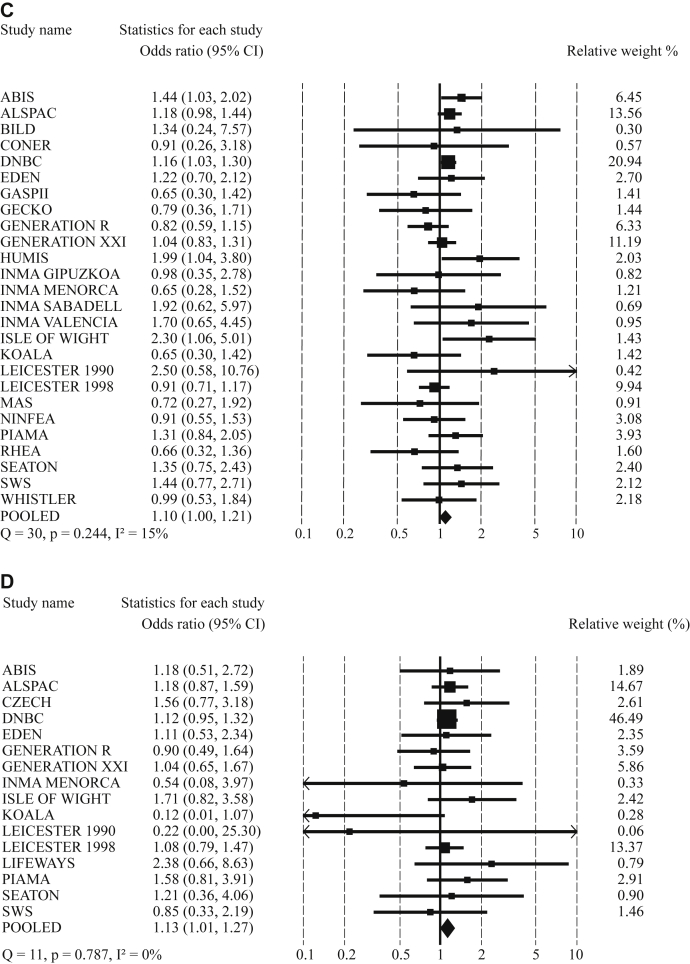
Methods: First, we performed an adjusted 1-stage random-effect meta-analysis to assess the combined associations of gestational age, birth weight, and infant weight gain with childhood asthma. Second, we performed an adjusted 2-stage random-effect meta-analysis to assess the associations of preterm birth (gestational age <37 weeks) and low birth weight (<2500 g) with childhood asthma outcomes.
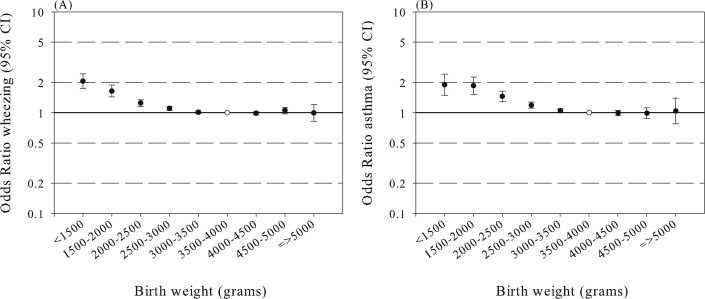
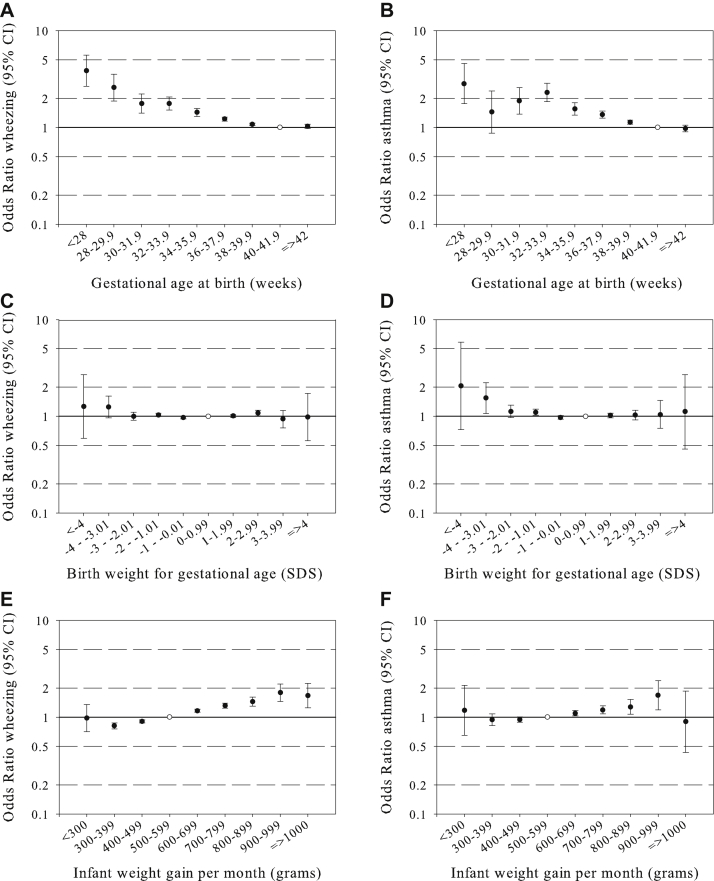
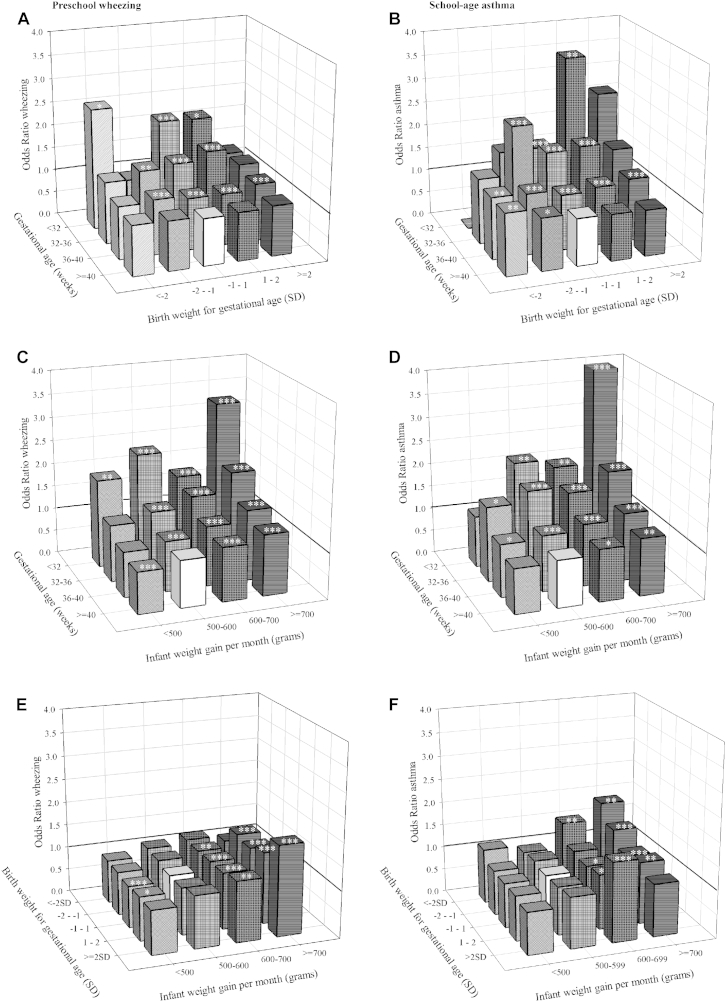
Results: Younger gestational age at birth and higher infant weight gain were independently associated with higher risks of preschool wheezing and school-age asthma (P < .05). The inverse associations of birth weight with childhood asthma were explained by gestational age at birth. Compared with term-born children with normal infant weight gain, we observed the highest risks of school-age asthma in children born preterm with high infant weight gain (odds ratio [OR], 4.47; 95% CI, 2.58-7.76). Preterm birth was positively associated with an increased risk of preschool wheezing (pooled odds ratio [pOR], 1.34; 95% CI, 1.25-1.43) and school-age asthma (pOR, 1.40; 95% CI, 1.18-1.67) independent of birth weight. Weaker effect estimates were observed for the associations of low birth weight adjusted for gestational age at birth with preschool wheezing (pOR, 1.10; 95% CI, 1.00-1.21) and school-age asthma (pOR, 1.13; 95% CI, 1.01-1.27).
Conclusion: Younger gestational age at birth and higher infant weight gain were associated with childhood asthma outcomes. The associations of lower birth weight with childhood asthma were largely explained by gestational age at birth.
Keywords: Gestational age; asthma; children; cohort studies; epidemiology; infant growth; low birth weight; wheezing.
Copyright © 2014 American Academy of Allergy, Asthma & Immunology. Published by Mosby, Inc. All rights reserved.
Figures
Comment in
-
Early-life weight gain, prematurity, and asthma development.J Allergy Clin Immunol. 2014 May;133(5):1330-1. doi: 10.1016/j.jaci.2014.03.005. J Allergy Clin Immunol. 2014. PMID: 24766877 No abstract available.
References
-
- Caudri D., Wijga A., Gehring U., Smit H.A., Brunekreef B., Kerkhof M. Respiratory symptoms in the first 7 years of life and birth weight at term: the PIAMA Birth Cohort. Am J Respir Crit Care Med. 2007;175:1078–1085. - PubMed
-
- Kindlund K., Thomsen S.F., Stensballe L.G., Skytthe A., Kyvik K.O., Backer V. Birth weight and risk of asthma in 3-9-year-old twins: exploring the fetal origins hypothesis. Thorax. 2010;65:146–149. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
