

Measles resurgence in southern Africa: challenges to measles elimination
- PMID: 24530936
- PMCID: PMC10292670
- DOI: 10.1016/j.vaccine.2014.01.089
Measles resurgence in southern Africa: challenges to measles elimination
Abstract
Introduction: In seven southern African countries (Botswana, Lesotho, Malawi, Namibia, South Africa, Swaziland and Zimbabwe), following implementation of a measles mortality reduction strategy starting in 1996, the number of annually reported measles cases decreased sharply to less than one per million population during 2006-2008. However, during 2009-2010, large outbreaks occurred in these countries. In 2011, a goal for measles elimination by 2020 was set in the World Health Organization (WHO) African Region (AFR). We reviewed the implementation of the measles control strategy and measles epidemiology during the resurgence in the seven southern African countries.
Methods: Estimated coverage with routine measles vaccination, supplemental immunization activities (SIA), annually reported measles cases by country, and measles surveillance and laboratory data were analyzed using descriptive analysis.
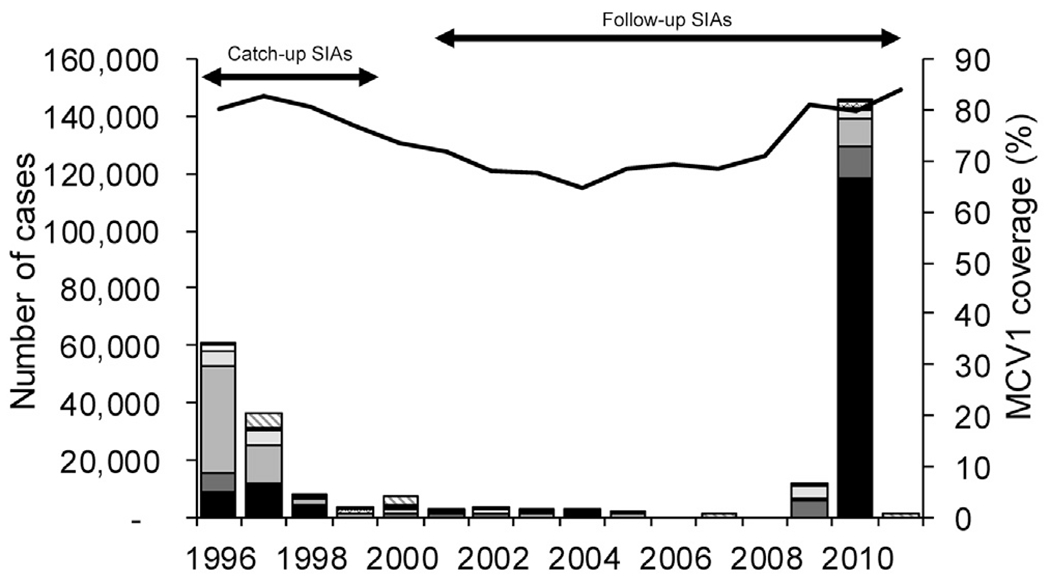
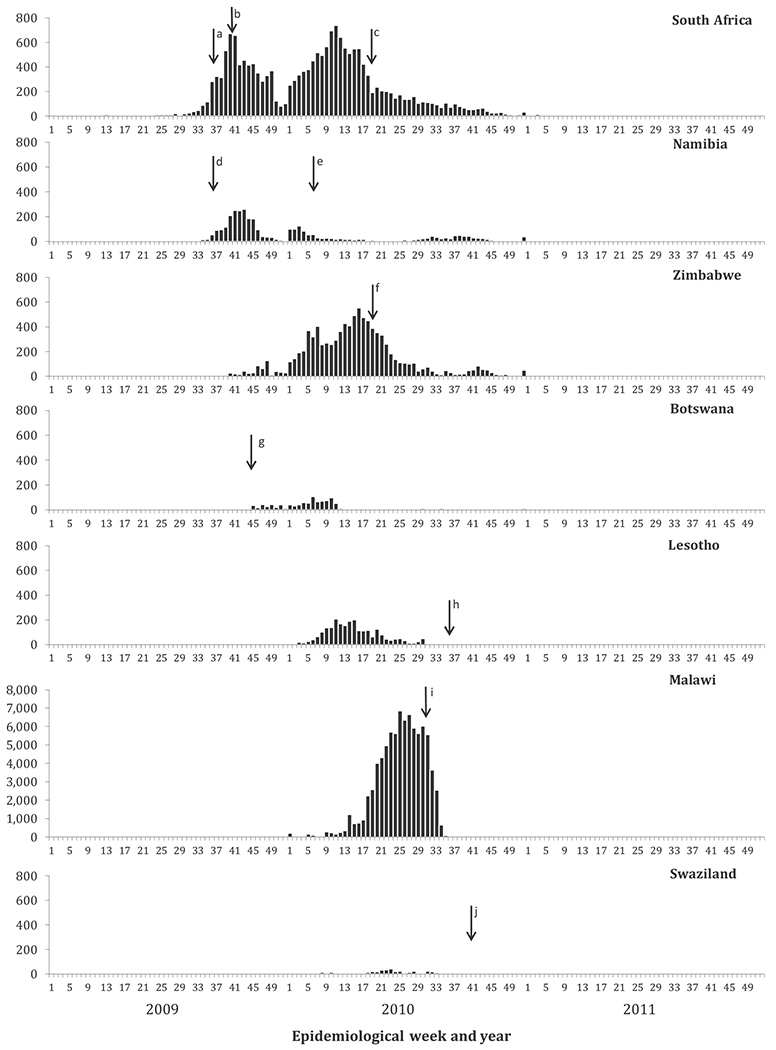
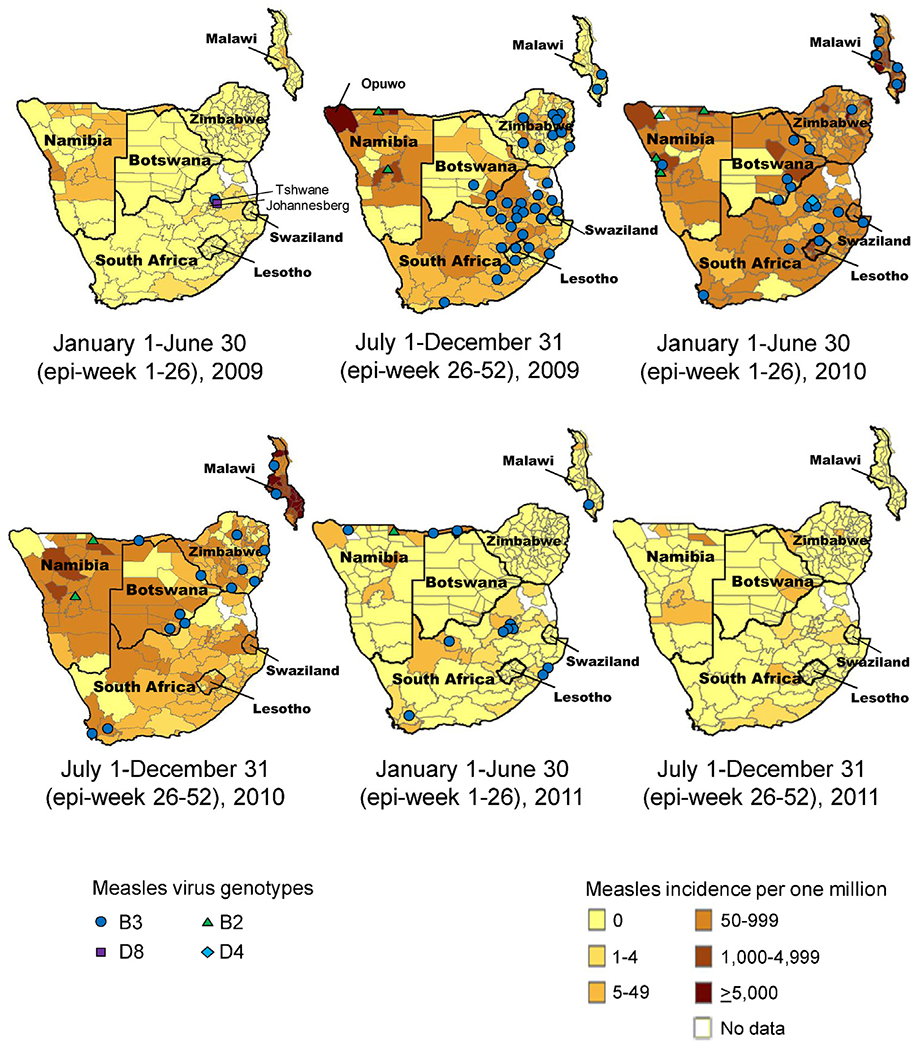
Results: In the seven countries, coverage with the routine first dose of measles-containing vaccine (MCV1) decreased from 80% to 65% during 1996-2004, then increased to 84% in 2011; during 1996-2011, 79,696,523 people were reached with measles vaccination during 45 SIAs. Annually reported measles cases decreased from 61,160 cases to 60 cases and measles incidence decreased to <1 case per million during 1996-2008. During 2009-2010, large outbreaks that included cases among older children and adults were reported in all seven countries, starting in South Africa and Namibia in mid-2009 and in the other five countries by early 2010. The measles virus genotype detected was predominantly genotype B3.
Conclusion: The measles resurgence highlighted challenges to achieving measles elimination in AFR by 2020. To achieve this goal, high two-dose measles vaccine coverage by strengthening routine immunization systems and conducting timely SIAs targeting expanded age groups, potentially including young adults, and maintaining outbreak preparedness to rapidly respond to outbreaks will be needed.
Keywords: Africa; Elimination; Immunization; Measles; Vaccination.
Published by Elsevier Ltd.
Conflict of interest statement
Conflicts of interest
We declare that we have no conflict of interest.
Figures
References
-
- Wolfson LJ, Strebel PM, Gacic-Dobo M, et al. Has the 2005 measles mortality reduction goal been achieved? A natural history modelling study. Lancet 2007;369(9557):191–200. - PubMed
-
- World Health Organization. Global vaccine action plan 2011–2020. Geneva: World Health Organization; 2013. http://www.who.int/immunization/global_vaccine_action_plan/GVAP_doc_2011... [accessed September 25, 2013].
-
- World Health Organization Regional Office for South-East Asia. Resolution of the WHO Regional Committee for South-East Asia. SEA/RC66/R5. Measles Elimination and Rubella/Congenital Rubella Syndrome Control; 2013.
-
- de Quadros CA, Olive JM, Hersh BS, et al. Measles elimination in the Americas, evolving strategies. JAMA 1996;275(3):224–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
