

Tamponade in surgery for retinal detachment associated with proliferative vitreoretinopathy
- PMID: 24532038
- PMCID: PMC3990035
- DOI: 10.1002/14651858.CD006126.pub3
Tamponade in surgery for retinal detachment associated with proliferative vitreoretinopathy
Update in
-
Tamponade in surgery for retinal detachment associated with proliferative vitreoretinopathy.Cochrane Database Syst Rev. 2020 May 13;5(5):CD006126. doi: 10.1002/14651858.CD006126.pub4. Cochrane Database Syst Rev. 2020. PMID: 32408387 Free PMC article.
Abstract
Background: Retinal detachment (RD) with proliferative vitreoretinopathy (PVR) often requires surgery to restore normal anatomy and to stabilize or improve vision. PVR usually occurs in association with recurrent RD (that is, after initial retinal re-attachment surgery) but occasionally may be associated with primary RD. Either way, a tamponade agent (gas or silicone oil) is needed during surgery to reduce the rate of postoperative recurrent RD.
Objectives: The objective of this review was to assess the relative safety and effectiveness of various tamponade agents used with surgery for retinal detachment (RD) complicated by proliferative vitreoretinopathy (PVR).
Search methods: We searched CENTRAL (which contains the Cochrane Eyes and Vision Group Trials Register) (The Cochrane Library 2013, Issue 5), Ovid MEDLINE, Ovid MEDLINE In-Process and Other Non-Indexed Citations, Ovid MEDLINE Daily, Ovid OLDMEDLINE (January 1946 to June 2013), EMBASE (January 1980 to June 2013), Latin American and Caribbean Literature on Health Sciences (LILACS) (January 1982 to June 2013), the metaRegister of Controlled Trials (mRCT) (www.controlled-trials.com), ClinicalTrials.gov (www.clinicaltrials.gov) and the WHO International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/search/en). We did not use any date or language restrictions in the electronic searches for trials. We last searched the electronic databases on 26 June 2013.
Selection criteria: We included randomized controlled trials (RCTs) of participants undergoing surgery for RD associated with PVR that compared various tamponade agents.
Data collection and analysis: Two review authors screened the search results independently. We used the standard methodological procedures expected by The Cochrane Collaboration.
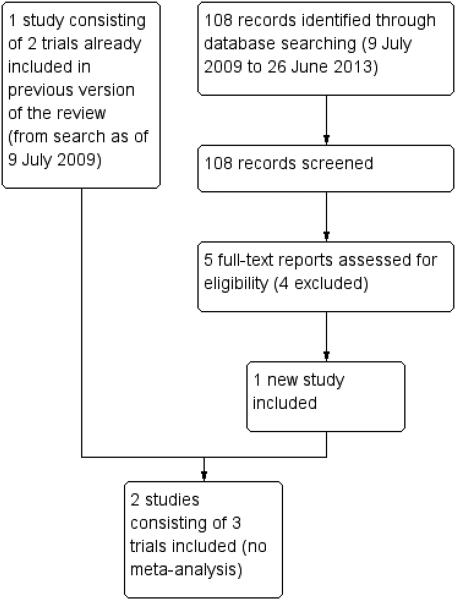
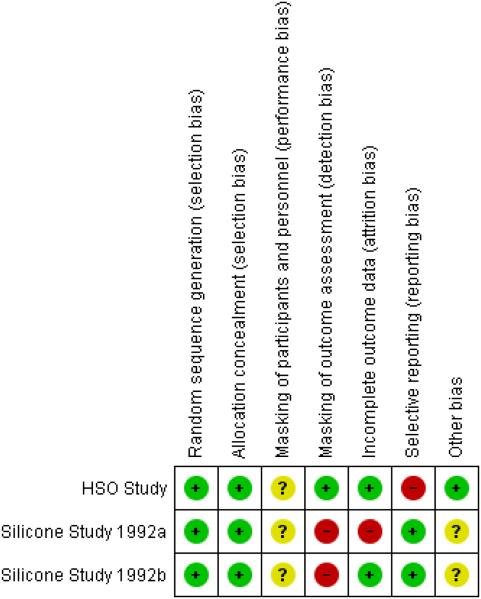
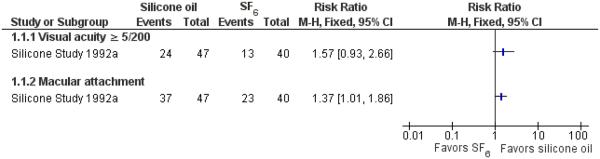
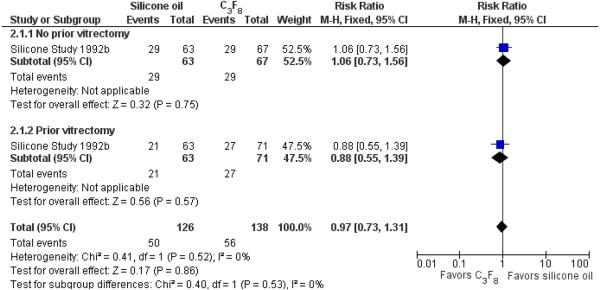
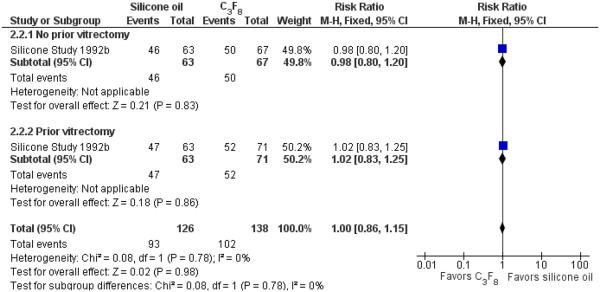
Main results: The review included 516 participants from three RCTs. One study was conducted in the USA and consisted of two trials: the first trial randomized 151 adults to receive either silicone oil or sulfur hexafluoride (SF6) gas tamponades; and the second trial randomized 271 adults to receive either silicone oil or perfluropropane (C3F8) gas tamponades. The third trial was a multi-center international trial and randomized 94 participants (age range not specified) to receive heavy silicone oil (a mixture of perfluorohexyloctane (F6H8) and silicone oil) versus standard silicone oil (either 1000 centistokes or 5000 centistokes, per the surgeon's preference).In participants with RD associated with PVR, outcomes after pars plana vitrectomy and infusion of either silicone oil, perfluropropane gas, or sulfur hexafluoride gas appeared comparable for a broad variety of cases. There were no significant differences between silicone oil and perfluoropropane gas in terms of the proportion of participants achieving at least 5/200 visual acuity (risk ratio (RR) 0.97; 95% confidence interval (CI) 0.73 to 1.31) or achieving macular attachment (RR 1.00; 95% CI 0.86 to 1.15) at a minimum of one year. Although sulfur hexafluoride gas was reported to be associated with significantly worse anatomic and visual outcomes than was silicone oil at one year (quantitative data not reported), there were no significant differences between silicone oil and sulfur hexafluoride gas in terms of achieving at least 5/200 visual acuity at two years (RR 1.57; 95% CI 0.93 to 2.66). For macular attachment, participants treated with silicone oil received significantly more favourable outcomes than did participants who received sulfur hexafluoride at both one year (quantitative data not reported) and two years (RR 1.37; 95% CI 1.01 to 1.86). The first two trials did not perform any sample size calculation or power detection. In the third trial, which had a power of 80% to detect differences, heavy silicone oil was not shown to be superior to standard silicone oil. There were no significant differences between standard silicone oil and heavy silicone oil in the change in visual acuity at one year using adjusted mean logMAR visual acuity (mean difference -0.03 logMAR; 95% CI -0.35 to 0.29). Adverse events were not reported for the first two trials. For the third trial, only the total number of adverse events was reported, and adverse events for each group were not specified. Of the 94 participants, four died, 26 had recurrent retinal detachment, 22 developed glaucoma, four developed a cataract, and two had capsular fibrosis.All three trials employed adequate methods for random sequence generation and allocation concealment. None of the trials employed masking of participants and surgeons, and only the third trial masked outcome assessors. The first trial had a large portion of participants excluded from the final analyses, while the other two trials were at low risk of attrition bias. All trials appear to be free of reporting bias. The first two trials were funded by the National Eye Institute, and the third trial was funded by the German Research Foundation.
Authors' conclusions: The use of either perfluropropane or standard silicone oil appears reasonable for most patients with RD associated with PVR. Because there do not appear to be any major differences in outcomes between the two agents, the choice of a tamponade agent should be individualized for each patient. Heavy silicone oil, which is not available for routine clinical use in the USA, has not demonstrated evidence of superiority over standard silicone oil.
Figures

Update of
-
Tamponade in surgery for retinal detachment associated with proliferative vitreoretinopathy.Cochrane Database Syst Rev. 2009 Oct 7;(4):CD006126. doi: 10.1002/14651858.CD006126.pub2. Cochrane Database Syst Rev. 2009. Update in: Cochrane Database Syst Rev. 2014 Feb 14;(2):CD006126. doi: 10.1002/14651858.CD006126.pub3. PMID: 19821354 Free PMC article. Updated.
References
-
-
References to studies included in this review
-
-
-
HSO Study {published data only}
-
-
- Joussen AM, Kirchhof B, Schrage N, Ocklenburg C, Hilgers RD. Heavy silicone oil versus standard silicone oil as vitreous tamponade in inferior PVR (HSO Study): design issues and implications. Acta Ophthalmologica Scandinavica. 2007;85(6):623–30. - PubMed
-
- Joussen AM, Rizzo S, Kirchhof B, Schrage N, Li X, Lente C, HSO-Study Group Heavy silicone oil versus standard silicone oil in as vitreoustamponade in inferior PVR (HSO Study): interim analysis. Acta Ophthalmologica. 2011;89(6):e483–9. - PubMed
-
-
Silicone Study 1992a {published data only}
-
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous