

Statistical SPECT processing in MRI-negative epilepsy surgery
- PMID: 24532274
- PMCID: PMC3963002
- DOI: 10.1212/WNL.0000000000000209
Statistical SPECT processing in MRI-negative epilepsy surgery
Abstract
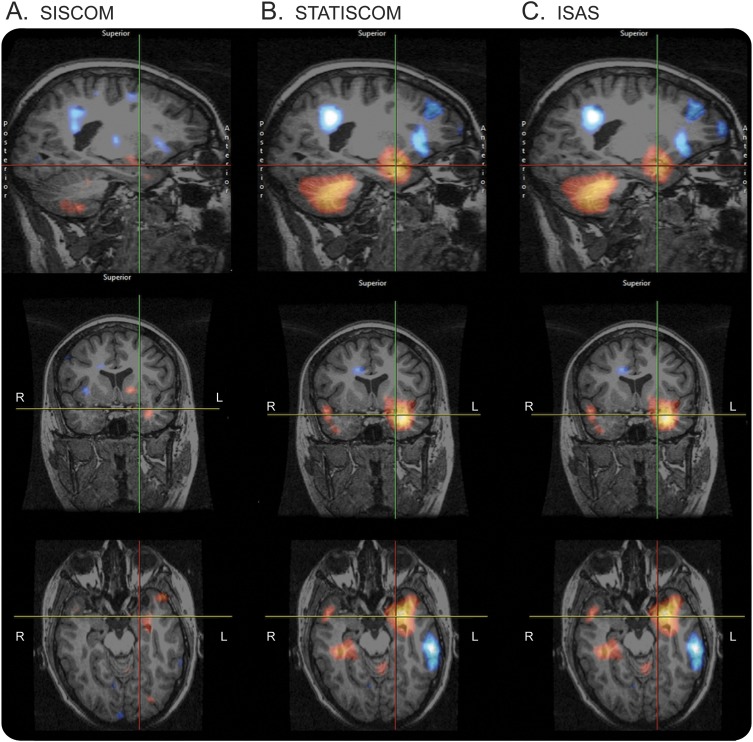
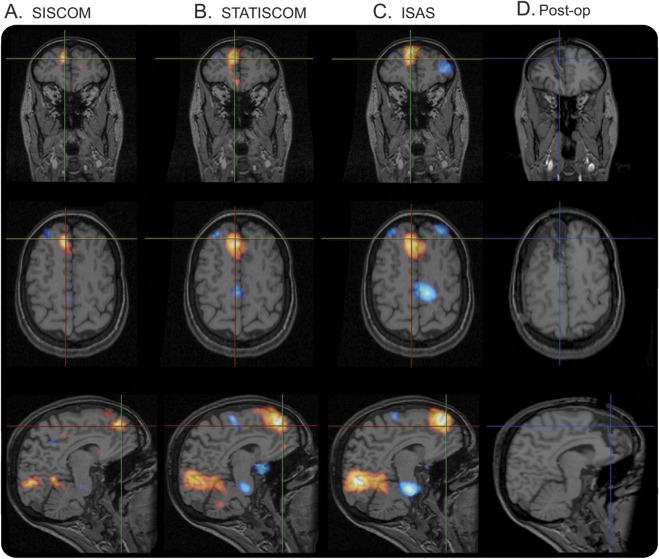
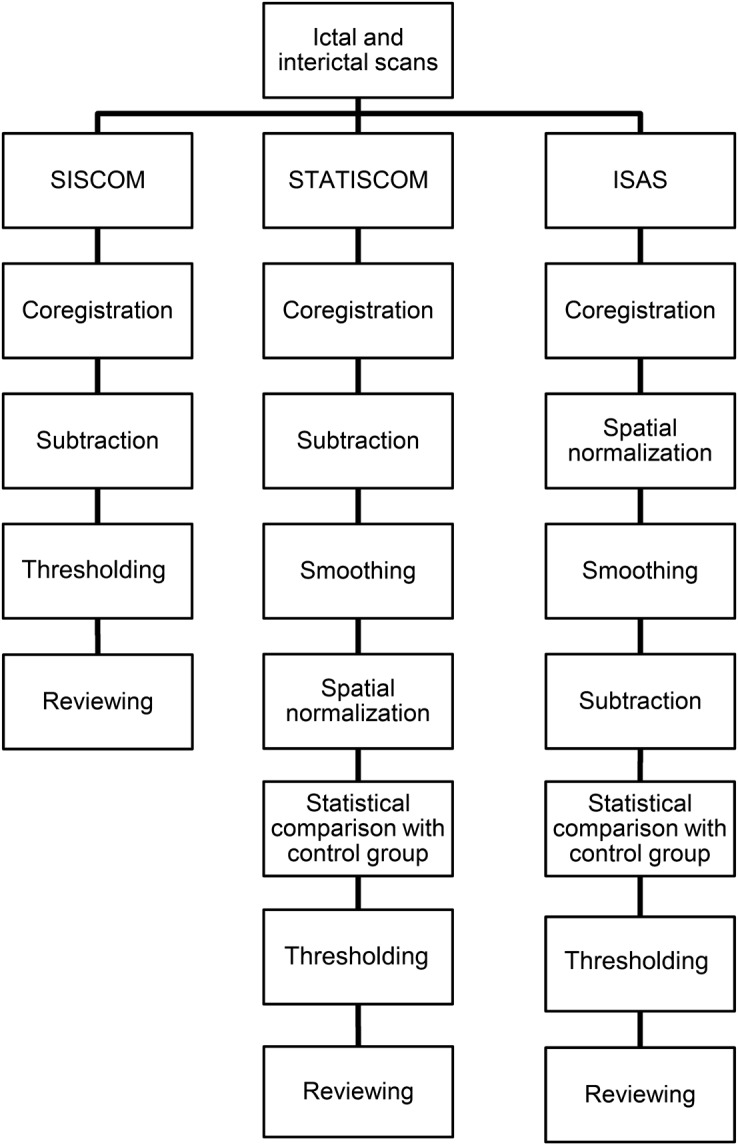
Objective: To evaluate the benefit of statistical SPECT processing over traditional subtraction methods, we compared ictal-interictal SPECT analyzed by statistical parametric mapping (SPM) (ISAS), statistical ictal SPECT coregistered to MRI (STATISCOM), and subtraction ictal-interictal SPECT coregistered with MRI (SISCOM) in patients with MRI-negative focal temporal lobe epilepsy (nTLE) and extratemporal lobe epilepsy (nETLE).
Methods: We retrospectively identified 49 consecutive cases of drug-resistant focal epilepsy that had a negative preoperative MRI and underwent interictal and ictal SPECT prior to resective epilepsy surgery. Interictal and ictal SPECT scans were analyzed using SISCOM, ISAS, and STATISCOM to create hyperperfusion and hypoperfusion maps for each patient. Reviewers blinded to clinical data and the SPECT analysis method marked the site of probable seizure origin and indicated their confidence in the localization.
Results: In nTLE and nETLE, the hyperperfusions detected by STATISCOM (71% nTLE, 57% nETLE) and ISAS (67% nTLE, 53% nETLE) were more often colocalized with surgery resection site compared to SISCOM (38% nTLE, 36% nETLE). In nTLE, localization of the hyperperfusion to the region of surgery was associated with an excellent outcome for STATISCOM (p = 0.005) and ISAS (p = 0.027), but not in SISCOM (p = 0.071). This association was not present in nETLE for any method.
Conclusion: In an unselected group of patients with normal MRI and focal epilepsy, SPM-based methods of SPECT processing showed better localization of SPECT hyperperfusion to surgical resection site and higher interobserver agreement compared to SISCOM. These results show the benefit of statistical SPECT processing methods and further highlight the challenge of nETLE.
Figures
Comment in
-
Resecting without detecting the lesion in extratemporal lobe epilepsy?Neurology. 2014 Mar 18;82(11):910-1. doi: 10.1212/WNL.0000000000000225. Epub 2014 Feb 14. Neurology. 2014. PMID: 24532278
References
-
- Sylaja PN, Radhakrishnan K, Kesavadas C, Sarma PS. Seizure outcome after anterior temporal lobectomy and its predictors in patients with apparent temporal lobe epilepsy and normal MRI. Epilepsia 2004;45:803–808 - PubMed
-
- Jayakar P, Dunoyer C, Dean P, et al. Epilepsy surgery in patients with normal or nonfocal MRI scans: integrative strategies offer long-term seizure relief. Epilepsia 2008;49:758–764 - PubMed
-
- Holmes M, Born D. Outcome after surgery in patients with refractory temporal lobe epilepsy and normal MRI. Seizure 2000;9:407–411 - PubMed
-
- Radhakrishnan K, So EL, Silbert PL, et al. Predictors of outcome of anterior temporal lobectomy for intractable epilepsy. Neurology 1998;51:465–471 - PubMed
-
- Siegel AM, Jobst BC, Thadani VM, et al. Medically intractable, localization-related epilepsy with normal MRI: presurgical evaluation and surgical outcome in 43 patients. Epilepsia 2001;42:883–888 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical