

Biomarkers in chronic obstructive pulmonary disease: confusing or useful?
- PMID: 24532968
- PMCID: PMC3923613
- DOI: 10.2147/COPD.S42362
Biomarkers in chronic obstructive pulmonary disease: confusing or useful?
Abstract
The field of biomarker research has almost reached unmanageable proportions in chronic obstructive pulmonary disease (COPD). The developments of new technology platforms have generated a huge information data base, both cross sectionally and increasingly, longitudinally. The knowledge emerging provides an enormous potential for understanding the disease pathophysiology, for developing markers specific for long-term outcomes, and for developing new therapeutic strategies. However, the excitement must be tempered with an understanding of the limitations of the data collection techniques, and of the variations in disease state, activity, impact, and progression. Nevertheless, the most crucial aspect in interpreting the current literature is the recognition of the relatively superficial characterization of what is a complex group of pathological processes with a common end point of airflow limitation. The current review explores some of these issues together with those areas where real progress appears to have been made, and provides caution on interpretation.
Keywords: emphysema; inflammation; secretions; technology platforms.
Figures
References
-
- Cote CG. Surrogates of mortality in chronic obstructive pulmonary disease. Am J Med. 2006;119(10 Suppl 1):S54–S62. - PubMed
-
- Clark KD, Wardrobe-Wong N, Elliott JJ, Gill PT, Tait NP, Snashall PD. Patterns of lung disease in a “normal” smoking population: are emphysema and airflow obstruction found together? Chest. 2001;120(3):743–747. - PubMed
-
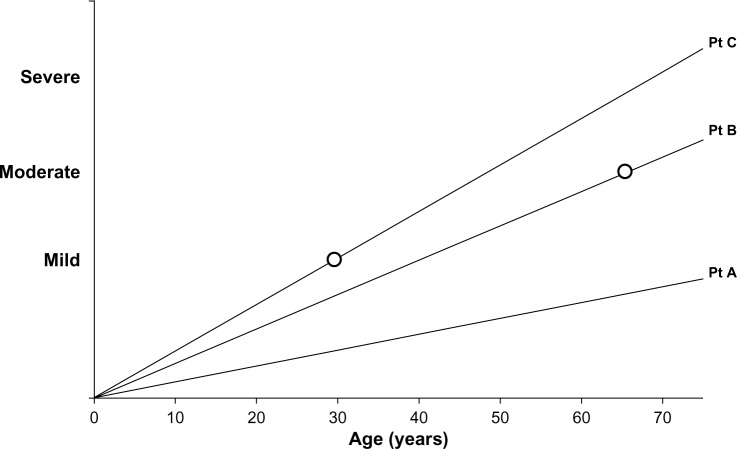
- Jones PW. Health status and the spiral of decline. COPD. 2009;6(1):59–63. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
