

Predictors of critical care needs after IV thrombolysis for acute ischemic stroke
- PMID: 24533130
- PMCID: PMC3922971
- DOI: 10.1371/journal.pone.0088652
Predictors of critical care needs after IV thrombolysis for acute ischemic stroke
Abstract
Background and purpose: Intravenous (IV) tissue plasminogen activator (tPA) is the only Food and Drug Administration (FDA)-approved treatment for acute ischemic stroke. Post tPA patients are typically monitored in an intensive care unit (ICU) for at least 24 hours. However, rigorous evidence to support this practice is lacking. This study evaluates factors that predict ICU needs after IV thrombolysis.
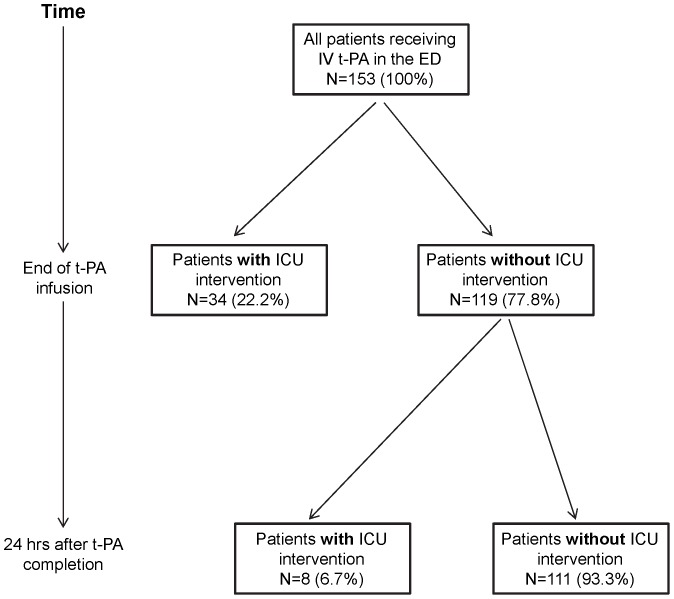
Methods: A retrospective chart review was performed for 153 patients who received intravenous tPA for acute ischemic stroke. Data on stroke risk factors, physiologic parameters on presentation, and stroke severity were collected. The timing and nature of an intensive care intervention, if needed, was recorded. Using multivariable logistic regression, we determined factors associated with requiring ICU care.
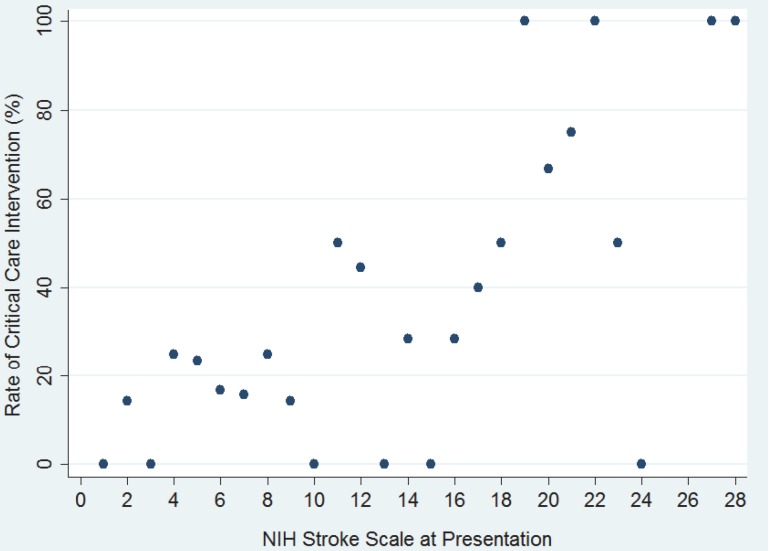
Results: African American race (Odds Ratio [OR] 8.05, 95% Confidence Interval [CI] 2.65-24.48), systolic blood pressure, and National Institutes of Health Stroke Scale (NIHSS) (OR 1.20 per point increase, 95% CI 1.09-1.31) were predictors of utilization of ICU resources. Patients with an NIHSS≥10 had a 7.7 times higher risk of requiring ICU resources compared to patients who presented with an NIHSS<10 (p<0.001). Most patients with ICU needs developed them prior to the end of tPA infusion (81.0%, 95% CI 68.8-93.1). Only 7% of patients without ICU needs by the end of the tPA infusion went on to require ICU care later on. These patients were more likely to have diabetes mellitus and had significantly higher NIHSS compared to patients without further ICU needs (mean NIHSS 17.3, 95% CI 11.5-22.9 vs. 9.2, 95% CI 7.7-9.6).
Conclusion: Race, NIHSS, and systolic blood pressure predict ICU needs following tPA for acute ischemic stroke. We propose that patients without ICU needs by the end of the tPA infusion might be safely monitored in a non-ICU setting if NIHSS at presentation is low.
Conflict of interest statement
Figures
References
-
- Mensah GA, Mendis S, Greenland K, MacKay J (2004) The atlas of heart disease and stroke. World Health Organization
-
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, et al. (2010) Executive summary: Heart disease and stroke statistics–2010 update: A report from the american heart association. Circulation 121: 948–954. - PubMed
-
- Demaerschalk BM, Hwang HM, Leung G (2010) US cost burden of ischemic stroke: A systematic literature review. Am J Manag Care 16: 525–533. - PubMed
-
- Hacke W, Donnan G, Fieschi C, Kaste M, von Kummer R, et al. (2004) Association of outcome with early stroke treatment: Pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet 363: 768–774. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
