

Left atrial dimension and traditional cardiovascular risk factors predict 20-year clinical cardiovascular events in young healthy adults: the CARDIA study
- PMID: 24534011
- PMCID: PMC4215562
- DOI: 10.1093/ehjci/jeu018
Left atrial dimension and traditional cardiovascular risk factors predict 20-year clinical cardiovascular events in young healthy adults: the CARDIA study
Abstract
Aims: We investigated whether the addition of left atrial (LA) size determined by echocardiography improves cardiovascular risk prediction in young adults over and above the clinically established Framingham 10-year global CV risk score (FRS).
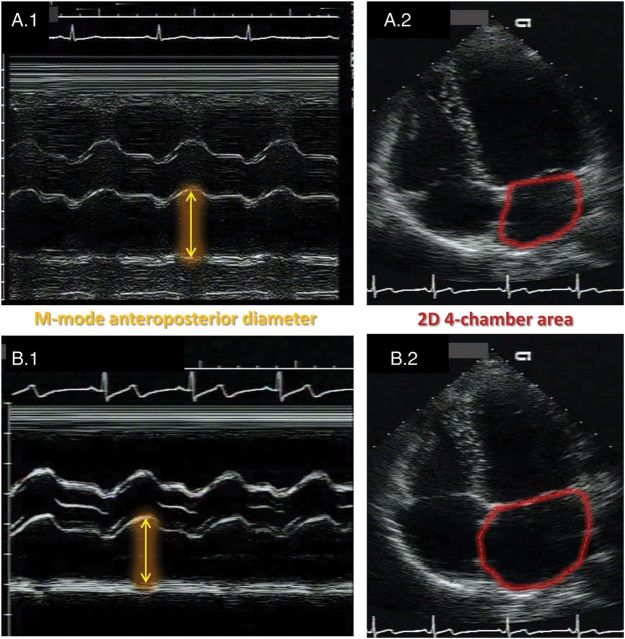
Methods and results: We included white and black CARDIA participants who had echocardiograms in Year-5 examination (1990-91). The combined endpoint after 20 years was incident fatal or non-fatal cardiovascular disease: myocardial infarction, heart failure, cerebrovascular disease, peripheral artery disease, and atrial fibrillation/flutter. Echocardiography-derived M-mode LA diameter (LAD; n = 4082; 149 events) and 2D four-chamber LA area (LAA; n = 2412; 77 events) were then indexed by height or body surface area (BSA). We used Cox regression, areas under the receiver operating characteristic curves (AUC), and net reclassification improvement (NRI) to assess the prediction power of LA size when added to calculated FRS or FRS covariates. The LAD and LAA cohorts had similar characteristics; mean LAD/height was 2.1 ± 0.3 mm/m and LAA/height 9.3 ± 2.0 mm(2)/m. After indexing by height and adjusting for FRS covariates, hazard ratios were 1.31 (95% CI 1.12, 1.60) and 1.43 (95% CI 1.13, 1.80) for LAD and LAA, respectively; AUC was 0.77 for LAD and 0.78 for LAA. When LAD and LAA were indexed to BSA, the results were similar but slightly inferior. Both LAD and LAA showed modest reclassification ability, with non-significant NRIs.
Conclusion: LA size measurements independently predict clinical outcomes. However, it only improves discrimination over clinical parameters modestly without altering risk classification. Indexing LA size by height is at least as robust as by BSA. Further research is needed to assess subgroups of young adults who may benefit from LA size information in risk stratification.
Keywords: Cardiovascular events; Echocardiography; Left atrial size; Young adults.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2014. For permissions please email: journals.permissions@oup.com.
Figures
References
-
- Greenland P, Alpert JS, Beller GA, Benjamin EJ, Budoff MJ, Fayad ZA, et al. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2010;122:e584–636. - PubMed
-
- D'Agostino RB, Sr, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117:743–53. - PubMed
-
- Pavlopoulos H, Nihoyannopoulos P. Left atrial size: a structural expression of abnormal left ventricular segmental relaxation evaluated by strain echocardiography. Eur J Echocardiogr. 2009;10:865–71. - PubMed
-
- Osranek M, Bursi F, Bailey KR, Grossardt BR, Brown RD, Jr, Kopecky SL, et al. Left atrial volume predicts cardiovascular events in patients originally diagnosed with lone atrial fibrillation: three-decade follow-up. Eur Heart J. 2005;26:2556–61. - PubMed
-
- Casaclang-Verzosa G, Gersh BJ, Tsang TS. Structural and functional remodeling of the left atrium: clinical and therapeutic implications for atrial fibrillation. J Am Coll Cardiol. 2008;51:1–11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
