

Serum uric acid and the risk of mortality during 23 years follow-up in the Scottish Heart Health Extended Cohort Study
- PMID: 24534458
- PMCID: PMC5590638
- DOI: 10.1016/j.atherosclerosis.2014.01.026
Serum uric acid and the risk of mortality during 23 years follow-up in the Scottish Heart Health Extended Cohort Study
Abstract
Background: Elevated uric acid is a prevalent condition with controversial health consequences. Observational studies disagree with regard to the relationship of uric acid with mortality, and with factors modifying this relationship.
Objective: We examined the association of serum uric acid with mortality in 15,083 participants in the Scottish Heart Health Extended Cohort (SHHEC) Study.
Methods: Serum uric acid was measured at study enrollment. Death was ascertained using both the Scottish death register and record linkage.
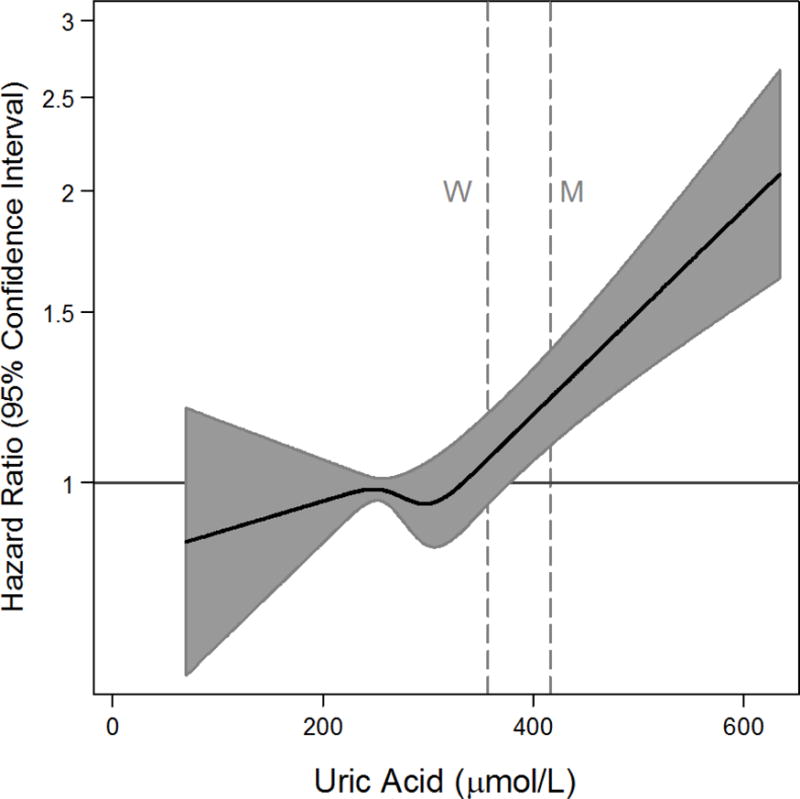
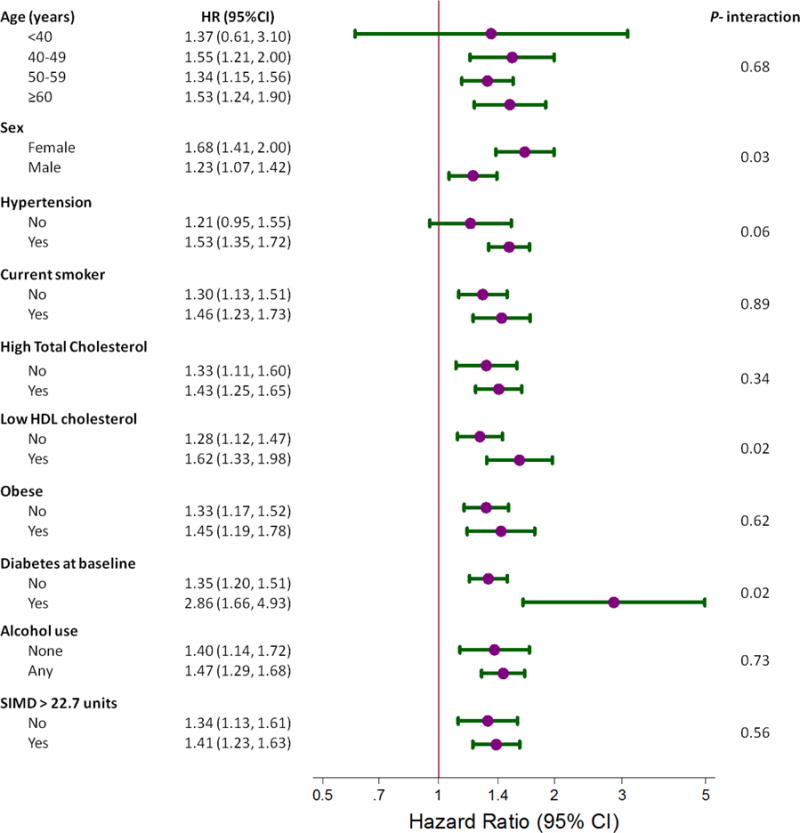
Results: During a median follow-up of 23 years, there were 3980 deaths. In Cox proportional hazards models with sexes combined, those in the highest fifth of uric acid had significantly greater mortality (HR 1.18, 95% CI: 1.06, 1.31) compared with the second fifth, after adjustment for traditional cardiovascular risk factors. This relationship was modified by sex (P-interaction=0.002) with adjusted HRs of 1.69 (95% CI: 1.40, 2.04) and 0.99 (95% CI: 0.86, 1.14) in women and men, respectively. Compared with the second fifth, the highest fifth of uric acid was most associated with kidney-related death (HR: 2.08, 95% CI: 1.31, 3.32).
Conclusion: Elevated uric acid is associated with earlier mortality, especially in women. Future studies should evaluate mechanisms for these interactions and explore the strong association with renal-related mortality.
Keywords: Cancer; Cardiovascular disease; Cohort; Hyperuricemia; Kidney disease; Mortality; Scottish Heart Health Extended Cohort (SHHEC); Uric acid.
Copyright © 2014 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
The authors have nothing to disclose and no relevant conflicts of interest.
Figures
References
-
- Nieto FJ, Iribarren C, Gross MD, Comstock GW, Cutler RG. Uric acid and serum antioxidant capacity: a reaction to atherosclerosis? Atherosclerosis. 2000;148:131–9. - PubMed
-
- Kim SY, De Vera MA, Choi HK. Gout and mortality. Clin Exp Rheumatol. 2008;26:S115–119. - PubMed
-
- Tomita M, Mizuno S, Yamanaka H, Hosoda Y, Sakuma K, Matuoka Y, et al. Does hyperuricemia affect mortality? A prospective cohort study of Japanese male workers. J Epidemiol. 2000;10:403–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
