

Atherosclerotic plaques occur in absence of intima-media thickening in both systemic sclerosis and systemic lupus erythematosus: a duplexsonography study of carotid and femoral arteries and follow-up for cardiovascular events
- PMID: 24548804
- PMCID: PMC3978872
- DOI: 10.1186/ar4489
Atherosclerotic plaques occur in absence of intima-media thickening in both systemic sclerosis and systemic lupus erythematosus: a duplexsonography study of carotid and femoral arteries and follow-up for cardiovascular events
Abstract
Introduction: The objective of this cross-sectional and retrospective cohort study was (1) to determine the usefulness of intima-media thickness (IMT) in contrast to plaque assessment, (2) to examine the value of additive femoral artery sonography and (3) to identify potential risk factors for atherosclerosis and incident cardiovascular events in systemic sclerosis (SSc) and systemic lupus erythematosus (SLE) patients.
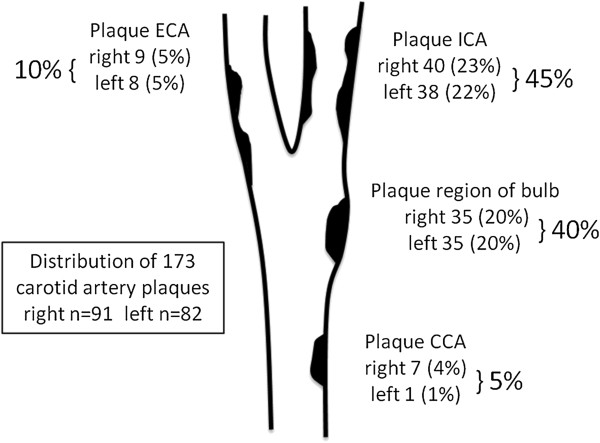
Methods: In this study, 90 SSc and 100 SLE patients were examined by duplexsonography. IMT was measured in common carotid and common femoral arteries, plaques were assessed in common, internal and external carotid and common, proximal superficial and deep femoral arteries. Different definitions of pathological IMT (pIMT) were compared with the presence of plaque. Results were evaluated in relation to traditional and non-traditional risk factors for baseline atherosclerosis (logistic regression) and their predictive value for cardiovascular events during follow-up (cox regression).
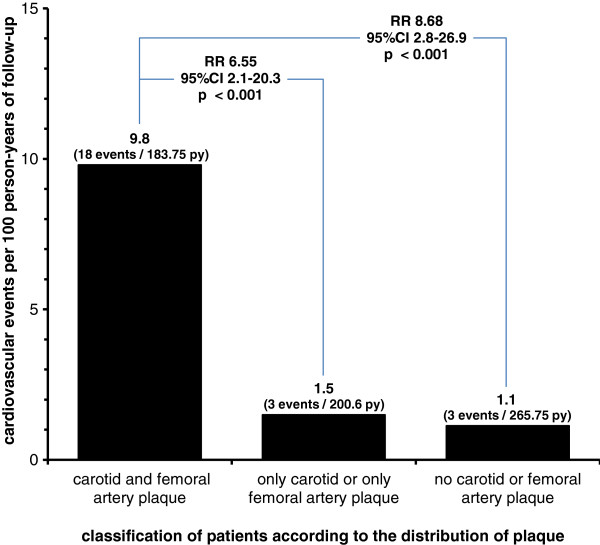
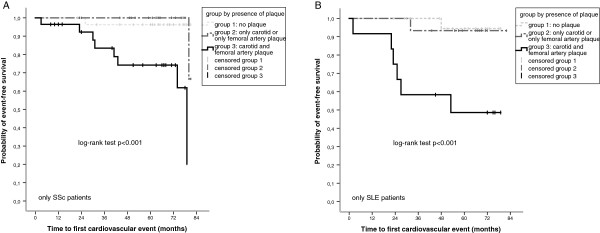
Results: Definite atherosclerosis occurred frequently without signs of subclinical atherosclerosis in both diseases: pIMT >0.9 mm was present in only 17/59 (28.9%) SSc and 13/49 (26.5%) SLE patients with already present atherosclerotic plaques. Using age-adjusted pIMT definitions, this rate was even lower (5.1-10.3% in SSc, 14.3-26.5% in SLE). Plaques were located only at the carotid or only at the femoral arteries in 26 (13.7%) and 24 (12.6%) patients, respectively. Age and nicotine pack-years were independently associated with atherosclerotic plaques in SLE and SSc patients, as well as the cumulative prednisolone dose in SSc subgroup, and ssDNA positive SLE patients had a lower risk for atherosclerotic plaque. During follow-up (available for 129/190 (67.9%) patients, 650 person-years), cardiovascular events occurred more often in patients with coronary heart disease (adjusted-hazards ratio (HR) 10.19, 95% confidence interval (CI) 3.04 to 34.17, P <0.001), male patients (adjusted-HR 8.78, 95% CI 2.73 to 28.19, P <0.001) and in patients with coexistent carotid and femoral plaques (adjusted-HR 5.92, 95% CI 1.55 to 22.67, P = 0.009). Patients with solely carotid or femoral plaque were not at higher risk.
Conclusion: Atherosclerotic plaque lesions can be found frequently in absence of intima-media thickening in both SSc and SLE patients. As well as routine sonography of carotid arteries, the sonography of femoral arteries is recommended to identify additional atherosclerotic lesions and to detect patients at a high risk for cardiovascular events.
Figures
References
-
- Anania C, Gustafsson T, Hua X, Su J, Vikström M, de Faire U, Heimbürger M, Jogestrand T, Frostegård J. Increased prevalence of vulnerable atherosclerotic plaques and low levels of natural IgM antibodies against phosphorylcholine in patients with systemic lupus erythematosus. Arthritis Res Ther. 2010;16:R214. doi: 10.1186/ar3193. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
