

Review
doi: 10.1503/cmaj.130989.
Epub 2014 Feb 18.
New treatments for metastatic melanoma
Affiliations
- PMID: 24549129
- PMCID: PMC4081198
- DOI: 10.1503/cmaj.130989
Item in Clipboard
Review
New treatments for metastatic melanoma
CMAJ.
.
No abstract available
Figures
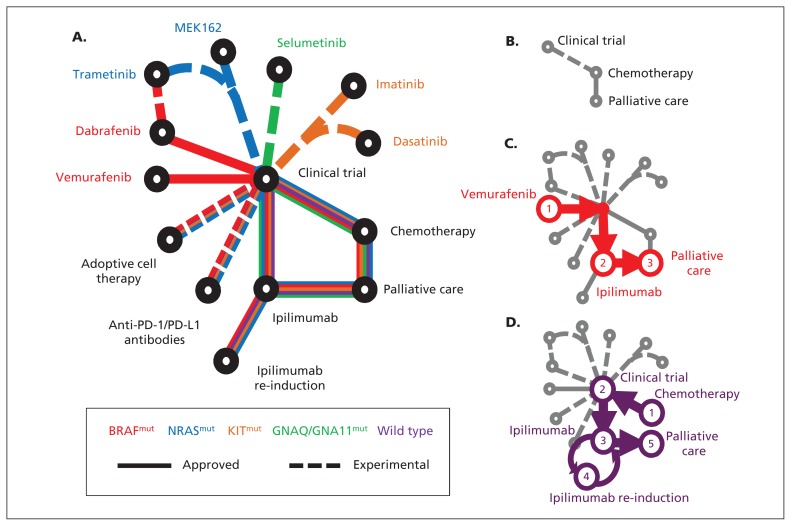
(A) Schematic of newly approved (solid lines) and experimental (dashed lines) treatments for patients with metastatic melanoma. The patient’s treatment is personalized according to the underlying driver mutation (e.g., NRAS-mutant in blue). (B) Historically, few treatments were available for melanoma. Examples of treatment progressions are shown for (C) patients with BRAF-mutant melanoma or (D) patients without an identifiable driver mutation (wild type). PD-1 = programmed cell death protein 1, PD-L1 = programmed cell death 1 ligand 1.
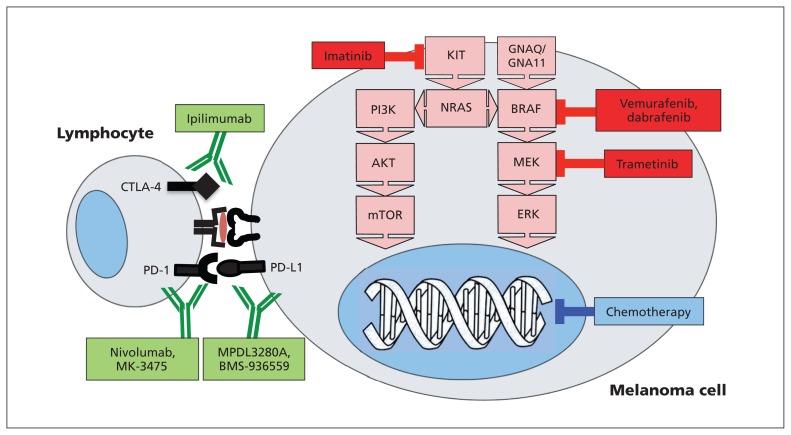
Immunotherapeutic antibodies target immune regulatory proteins on the surfaces of melanoma and lymphocyte cells (green), while kinase inhibitors (red) block mutated mitogen-activated protein kinase (MAPK) pathways. Traditional cytotoxic chemotherapy targets DNA replication (blue). CTLA-4 = cytotoxic T-lymphocyte–associated protein 4, ERK = extracellular signal-regulated kinase, MEK = mitogen-activated protein/ERK kinase, mTOR = mammalian target of rapamycin, PD-1 = programmed cell death protein 1, PD-L1 = programmed cell death 1 ligand 1.
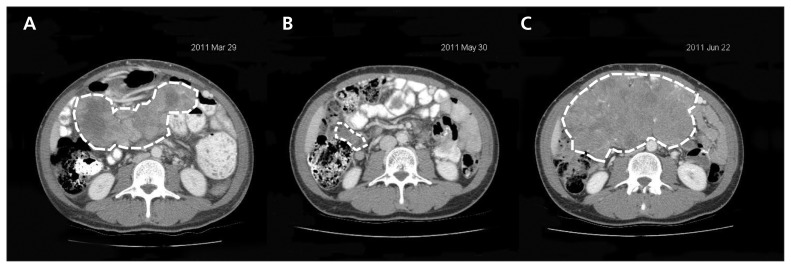
Responses to BRAF inhibitors can be dramatic, but relapses are almost invariable and can be equally rapid. Abdominal computed tomographic scans showing peritoneal metastases (dashed white lines) before treatment (A), and after two months (B) and three months (C) of treatment with vemurafenib.
References
-
- Barth A, Wanek LA, Morton DL. Prognostic factors in 1,521 melanoma patients with distant metastases. J Am Coll Surg 1995;181:193–201 - PubMed
-
- Cebon J, Gedye C, John T, et al. Immunotherapy of advanced or metastatic melanoma. Clin Adv Hematol Oncol 2007;5:994–1006 - PubMed
-
- Halliday GM, Patel A, Hunt MJ, et al. Spontaneous regression of human melanoma/nonmelanoma skin cancer: association with infiltrating CD4+ T cells. World J Surg 1995;19:352–8 - PubMed
-
- Curtin JA, Fridlyand J, Kageshita T, et al. Distinct sets of genetic alterations in melanoma. N Engl J Med 2005;353:2135–47 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical