

Can we treat select terrible triad injuries nonoperatively?
- PMID: 24549776
- PMCID: PMC4048392
- DOI: 10.1007/s11999-014-3518-9
Can we treat select terrible triad injuries nonoperatively?
Abstract
Background: While the majority of terrible triad elbow injuries (ulnohumeral dislocation with radial head and coronoid fractures) are managed surgically, nonoperative treatment may be appropriate in selected patients, but results with this approach have been limited by very small studies.
Questions/purposes: We assessed (1) functional outcomes using two validated questionnaires, (2) elbow ROM, strength, and stability, (3) the presence of union and arthritis on radiographs, and (4) complications among a group of patients managed nonoperatively for terrible triad injuries.
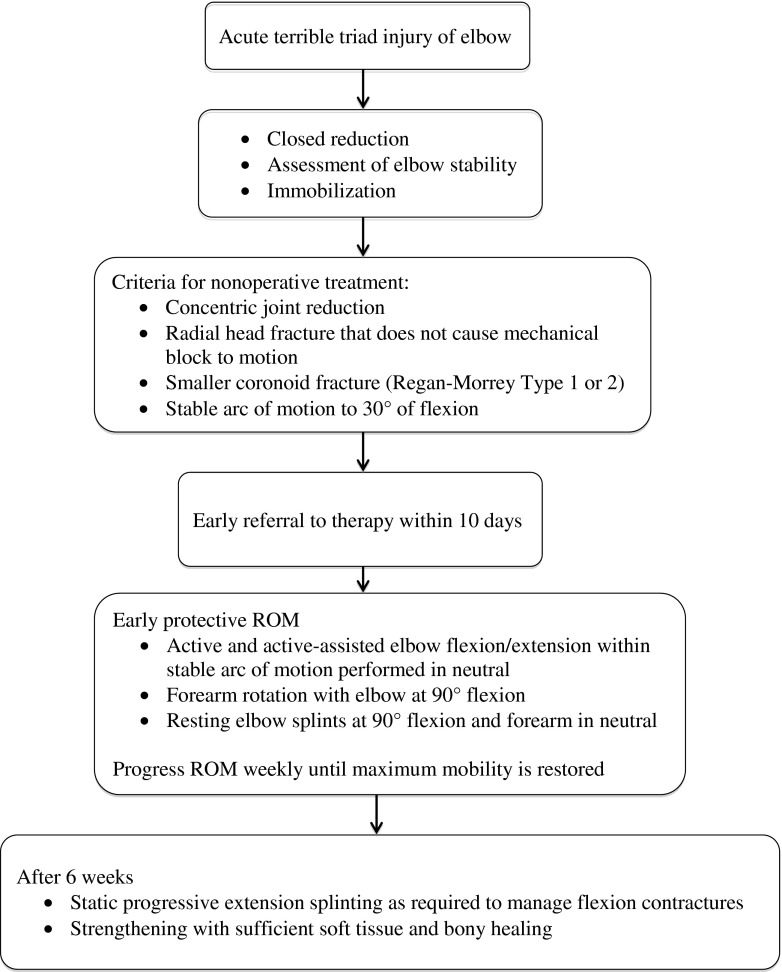
Methods: Between 2006 and 2012, we retrospectively identified 12 patients with terrible triad elbow injuries who were treated nonoperatively and met the following criteria: (1) a concentric joint reduction, (2) a radial head fracture that did not cause a mechanical block to rotation, (3) a smaller coronoid fracture (Regan-Morrey Type 1 or 2), and (4) a stable arc of motion to a minimum of 30° of extension to allow active motion within the first 10 days. Eleven patients were available for followup of at least 12 months after the injury (mean, 36 months; range, 12-90 months). Outcome measures included two patient-reported functional outcome measures (DASH, Mayo Elbow Performance Index [MEPI]), a standardized physical examination to record elbow ROM and stability, isometric strength measurements, and radiographic evidence of bony union and elbow arthrosis. Complications were also recorded.
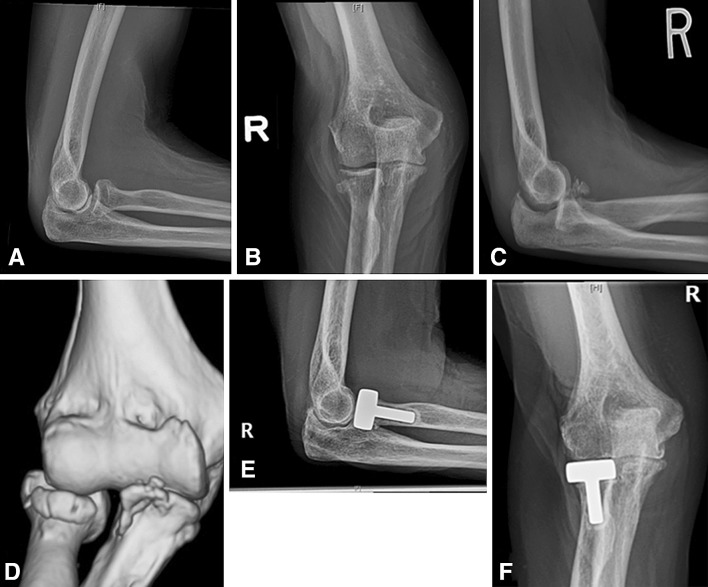
Results: At latest followup, mean ± SD DASH score was 8.0 ± 11.0 and mean MEPI score was 94 ± 9. Mean ROM of the affected elbow was 134° ± 5° flexion, 6° ± 8° extension, 87° ± 4° pronation, and 82° ± 10° supination. No instability was detected. Strength assessments demonstrated the following mean percentages of the contralateral, unaffected elbow: flexion 100%, extension 89%, pronation 79%, and supination 89%. Four patients had arthritic changes on radiographs that did not call for treatment as of latest followup. Complications included one patient who underwent surgical stabilization for early recurrent instability and another who underwent arthroscopic débridement for heterotopic bone.
Conclusions: In selected patients, nonoperative treatment of terrible triad injuries is an option that can provide good function and restore stable elbow ROM. However, nonoperative management requires close clinical and radiographic followup to monitor for any delayed elbow subluxation or fracture displacement.
Level of evidence: Level IV, therapeutic study. See Instructions for Authors for a complete description of levels of evidence.
Figures

References
-
- Broberg MA, Morrey BF. Results of treatment of fracture-dislocations of the elbow. Clin Orthop Relat Res. 1987;216:109–119. - PubMed
-
- Closkey RF, Goode JR, Kirschenbaum D, Cody RP. The role of the coronoid process in elbow stability: a biomechanical analysis of axial loading. J Bone Joint Surg Am. 2000;82:1749–1753. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
