

Hospital cardiac arrest resuscitation practice in the United States: a nationally representative survey
- PMID: 24550202
- PMCID: PMC4144704
- DOI: 10.1002/jhm.2174
Hospital cardiac arrest resuscitation practice in the United States: a nationally representative survey
Abstract
Background: In-hospital cardiac arrest (IHCA) outcomes vary widely between hospitals, even after adjusting for patient characteristics, suggesting variations in practice as a potential etiology. However, little is known about the standards of IHCA resuscitation practice among US hospitals.
Objective: To describe current US hospital practices with regard to resuscitation care.
Design: A nationally representative mail survey.
Setting: A random sample of 1000 hospitals from the American Hospital Association database, stratified into 9 categories by hospital volume tertile and teaching status (major teaching, minor teaching, and nonteaching).
Subjects: Surveys were addressed to each hospital's cardiopulmonary resuscitation (CPR) committee chair or chief medical/quality officer.
Measurements: A 27-item questionnaire.
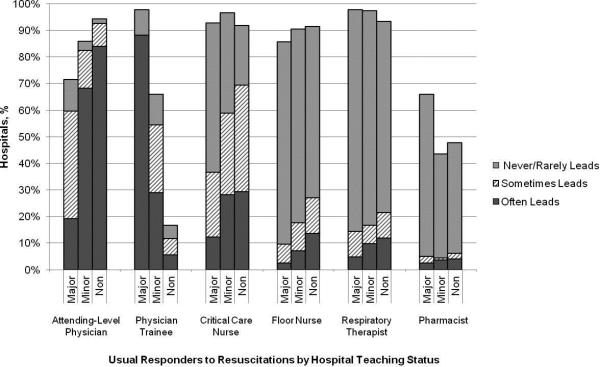
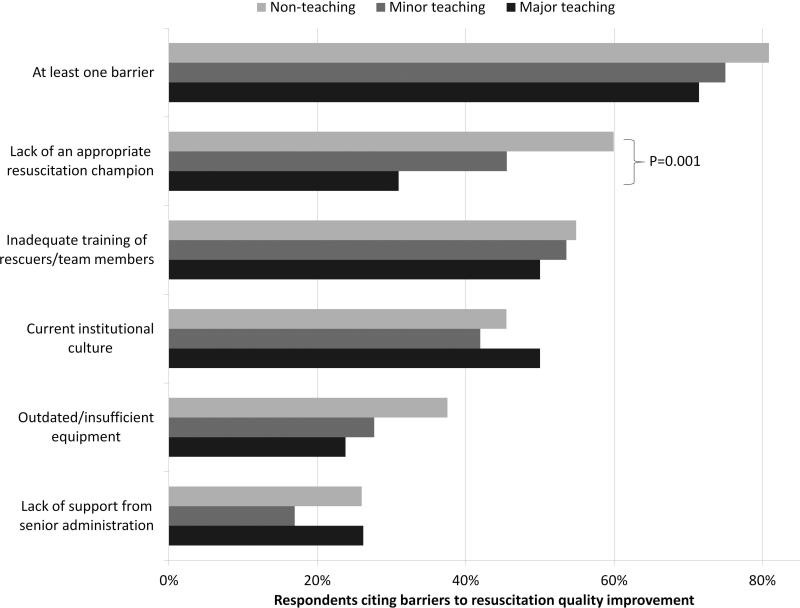
Results: Responses were received from 439 hospitals with a similar distribution of admission volume and teaching status as the sample population (P = 0.50). Of the 270 (66%) hospitals with a CPR committee, 23 (10%) were chaired by a hospitalist. High frequency practices included having a rapid response team (91%) and standardizing defibrillators (88%). Low frequency practices included therapeutic hypothermia and use of CPR assist technology. Other practices such as debriefing (34%) and simulation training (62%) were more variable and correlated with the presence of a CPR committee and/or dedicated personnel for resuscitation quality improvement. The majority of hospitals (79%) reported at least 1 barrier to quality improvement, of which the lack of a resuscitation champion and inadequate training were the most common.
Conclusions: There is wide variability among hospitals and within practices for resuscitation care in the United States with opportunities for improvement.
© 2014 Society of Hospital Medicine.
Figures
References
-
- Chan PS, Nichol G, Krumholz HM, Spertus JA, Nallamothu BK. Hospital variation in time to defibrillation after in-hospital cardiac arrest. Arch Intern Med. 2009 Jul 27;169(14):1265–1273. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
