

Prophylactic antibiotics to prevent cellulitis of the leg: economic analysis of the PATCH I & II trials
- PMID: 24551029
- PMCID: PMC3925077
- DOI: 10.1371/journal.pone.0082694
Prophylactic antibiotics to prevent cellulitis of the leg: economic analysis of the PATCH I & II trials
Abstract
Background: Cellulitis (erysipelas) is a recurring and debilitating bacterial infection of the skin and underlying tissue. We assessed the cost-effectiveness of prophylactic antibiotic treatment to prevent the recurrence of cellulitis using low dose penicillin V in patients following a first episode (6 months prophylaxis) and more recurrent cellulitis (12 months prophylaxis, or 6 months in those declining 12 months).
Methods: Within-trial cost-effectiveness analysis was conducted using the findings of two randomised placebo-controlled multicentre trials (PATCH I and PATCH II), in which patients recruited in the UK and Ireland were followed-up for up to 3 years. Incremental cost, reduction in recurrence, cost per recurrence prevented and cost/QALY were estimated. National unit and reference costs for England in 2010 were applied to resource use, exploring NHS and societal perspectives. A total of 397 patients from the two trials contributed to the analysis.
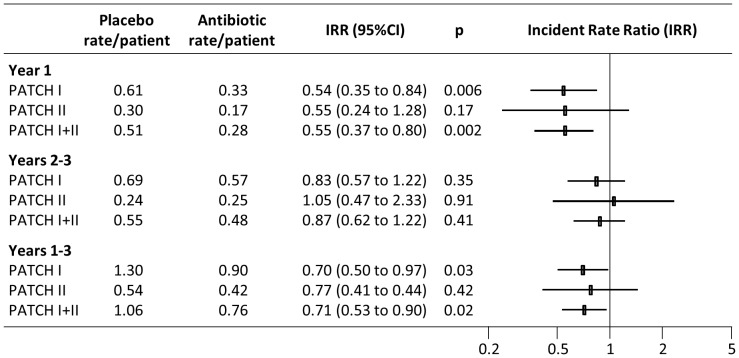
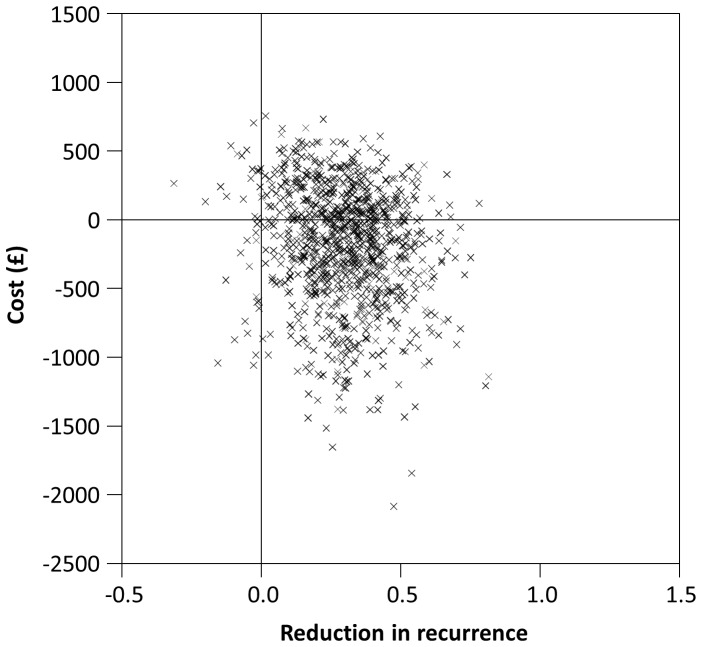
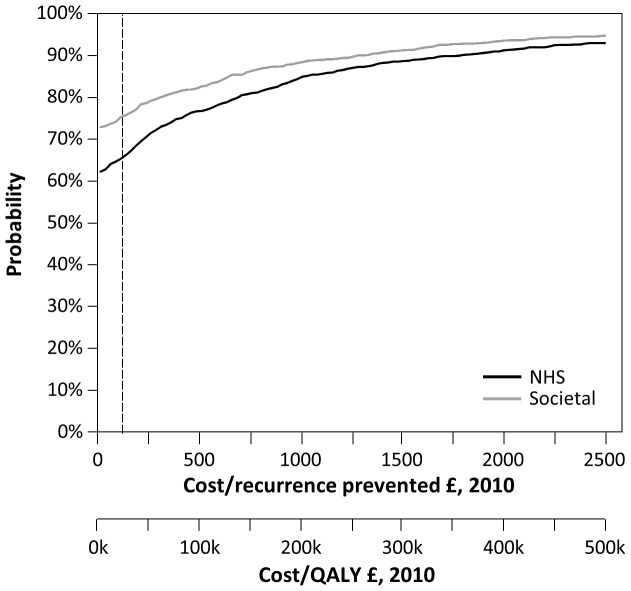
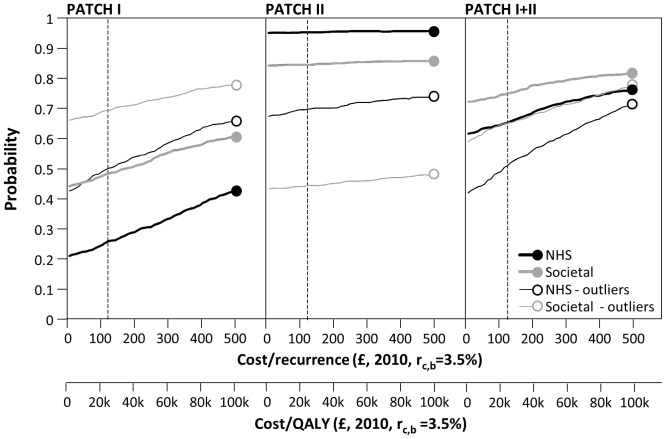
Results: There was a 29% reduction in the number of recurrences occurring within the trial (IRR: 0.71 95%CI: 0.53 to 0.90, p = 0.02), corresponding to an absolute reduction of recurrence of 0.31 recurrences/patient (95%CI: 0.05 to 0.59, p = 0.02). Incremental costs of prophylaxis suggested a small cost saving but were not statistically significant, comparing the two groups. If a decision-maker is willing to pay up to £25,000/QALY then there is a 66% probability of antibiotic prophylaxis being cost-effective from an NHS perspective, rising to 76% probability from a secondary, societal perspective.
Conclusion: Following first episode or recurrent cellulitis of the leg, prophylactic low dose penicillin is a very low cost intervention which, on balance, is effective and cost-effective at preventing subsequent attacks. Antibiotic prophylaxis reduces cellulitis recurrence by nearly a third but is not associated with a significant increase in costs.
Conflict of interest statement
Figures
References
-
- Cox NH (2006) Oedema as a risk factor for multiple episodes of cellulitis/erysipelas of the lower leg: a series with community follow-up. British Journal of Dermatology 155: 947–50. - PubMed
-
- Jeng A, Beheshti M, Li J, Nathan R (2010) The role of beta-hemolytic streptococci in causing diffuse, nonculturable cellulitis: a prospective investigation. Medicine 89: 217–26. - PubMed
-
- Bernard P, Bedane C, Mounier M, Denis F, Catanzano G, Bonnetblanc JM (1989) Streptococcal cause of erysipelas and cellulitis in adults. A microbiologic study using a direct immunofluorescence technique. Arch Dermatol. 125: 779–82. - PubMed
-
- Levell N, Wingfield C, Garioch J (2011) Severe lower limb cellulitis is best diagnosed by dermatologists and managed with shared care between primary and secondary care. British Journal of Dermatology 164: 1326–8. - PubMed
-
- Soo JK, Bicanic TA, Heenan S, Mortimer PS (2008) Lymphatic abnormalities demonstrated by lymphoscintigraphy after lower limb cellulitis. British Journal of Dermatology 158: 1350–53. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
