

The association between malaria and iron status or supplementation in pregnancy: a systematic review and meta-analysis
- PMID: 24551064
- PMCID: PMC3925104
- DOI: 10.1371/journal.pone.0087743
The association between malaria and iron status or supplementation in pregnancy: a systematic review and meta-analysis
Abstract
Introduction: Malaria prevention and iron supplementation are associated with improved maternal and infant outcomes. However, evidence from studies in children suggests iron may adversely modify the risk of malaria. We reviewed the evidence in pregnancy of the association between malaria and markers of iron status, iron supplementation or parenteral treatment.
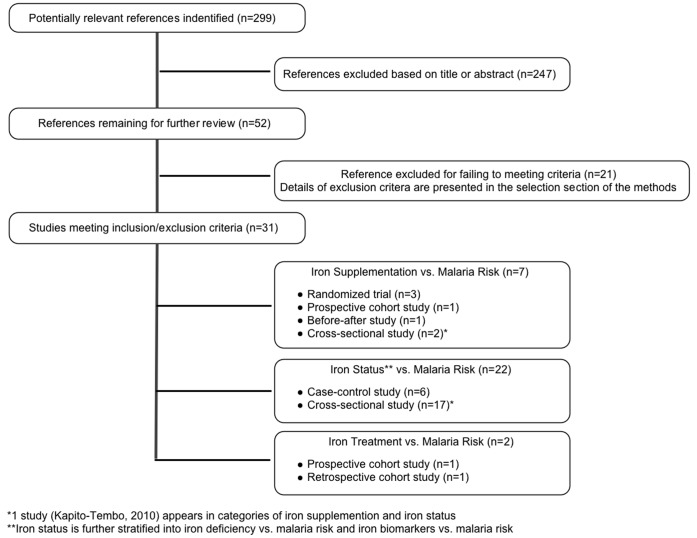
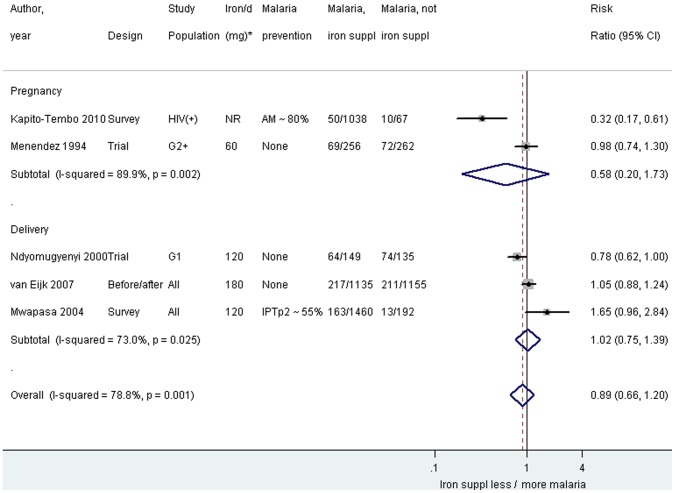
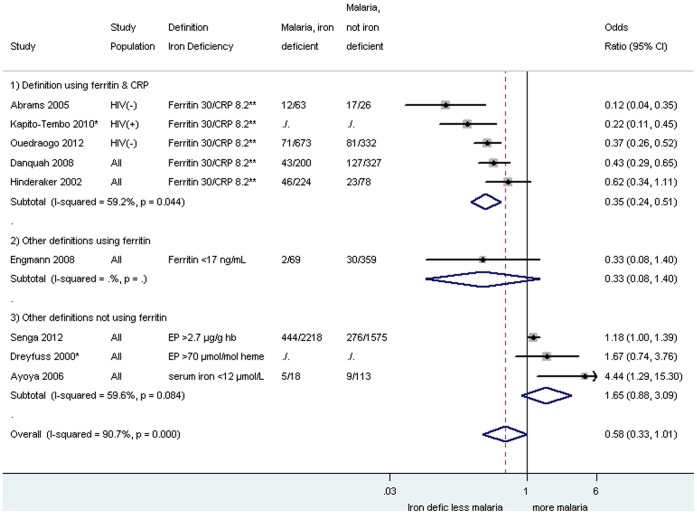
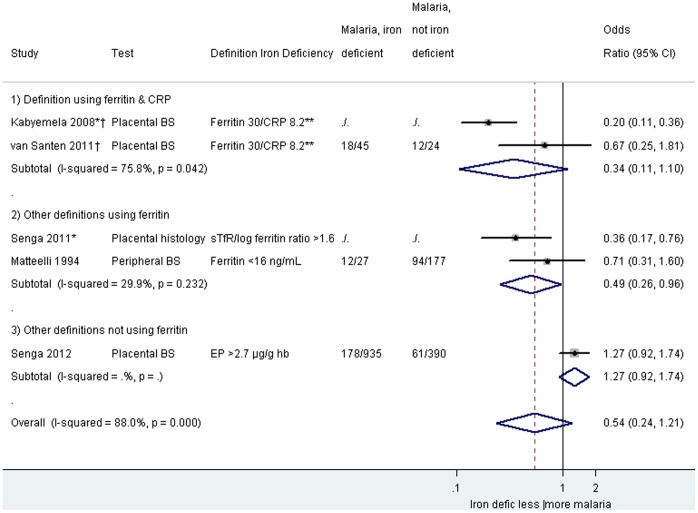
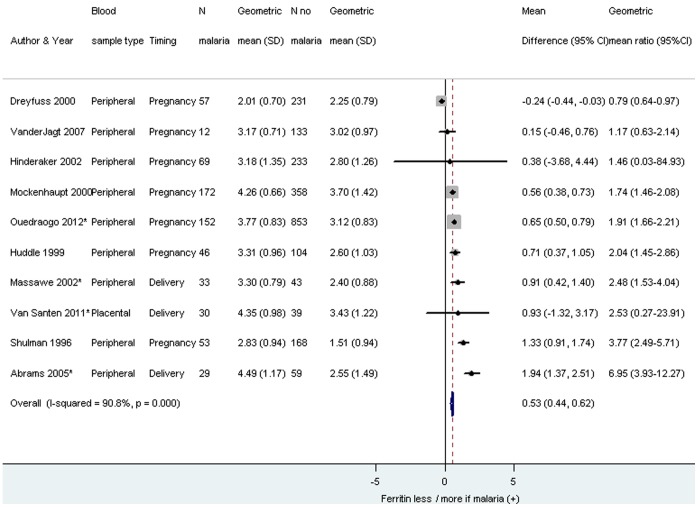
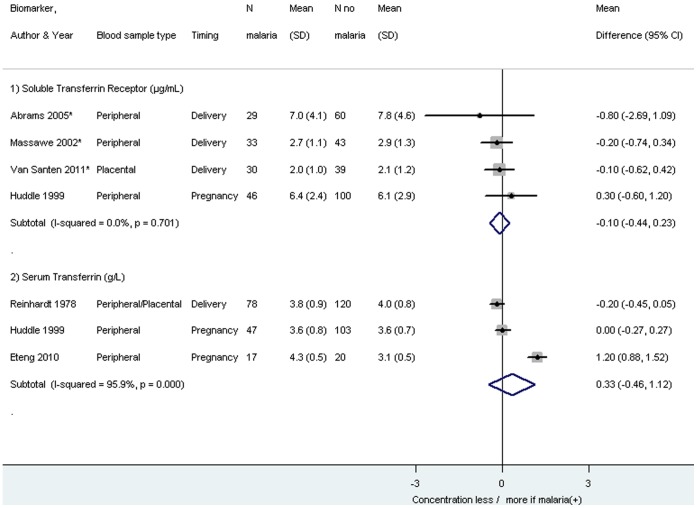
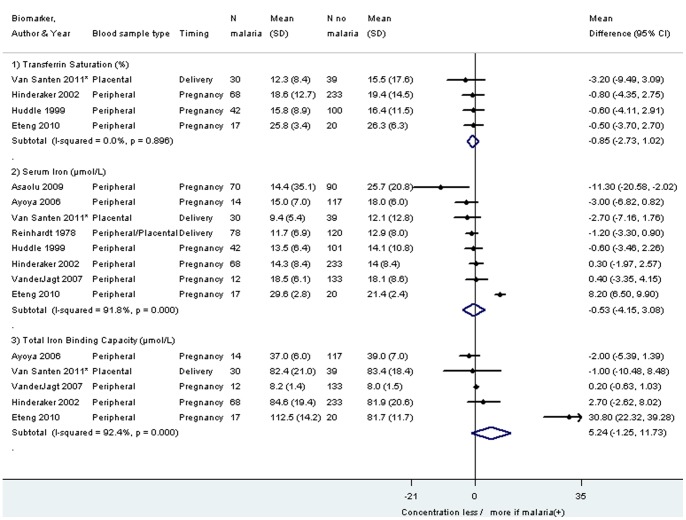
Methods and findings: We searched MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials, the Global Health Library, and the Malaria in Pregnancy library to identify studies that investigated the association between iron status, iron treatment or supplementation during pregnancy and malaria. Thirty one studies contributed to the analysis; 3 experimental and 28 observational studies. Iron supplementation was not associated with an increased risk of P. falciparum malaria during pregnancy or delivery in Africa (summary Relative Risk = 0.89, 95% Confidence Interval (CI) 0.66-1.20, I(2) = 78.8%, 5 studies). One study in Asia reported an increased risk of P. vivax within 30 days of iron supplementation (e.g. adjusted Hazard Ratio = 1.75, 95% CI 1.14-2.70 for 1-15 days), but not after 60 days. Iron deficiency (based on ferritin and C-reactive protein) was associated with lower odds for malaria infection (summary Odds Ratio = 0.35, 0.24-0.51, I(2) = 59.2%, 5 studies). With the exception of the acute phase protein ferritin, biomarkers of iron deficiency were generally not associated with malaria infection.
Conclusions: Iron supplementation was associated with a temporal increase in P vivax, but not with an increased risk of P. falciparum; however, data are insufficient to rule out the potential for an increased risk of P. falciparum. Iron deficiency was associated with a decreased malaria risk in pregnancy only when measured with ferritin. Until there is more evidence, it is prudent to provide iron in combination with malaria prevention during pregnancy.
Conflict of interest statement
Figures
References
-
- Gilles HM, Williams EJ, Ball PA (1964) Hookworm Infection and Anaemia. An Epidemiological, Clinical, and Laboratory Study. Q J Med 33: 1–24. - PubMed
-
- Rush D (2000) Nutrition and maternal mortality in the developing world. Am J Clin Nutr 72: 212S–240S. - PubMed
-
- Gillespie S (1998) Major issues in the control of iron deficiency. New York, USA: The Micronutrient Initiative.
-
- Bundy DA, de Silva NR (1998) Can we deworm this wormy world? Br Med Bull 54: 421–432. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
