

A randomized trial of bevacizumab for newly diagnosed glioblastoma
- PMID: 24552317
- PMCID: PMC4201043
- DOI: 10.1056/NEJMoa1308573
A randomized trial of bevacizumab for newly diagnosed glioblastoma
Abstract
Background: Concurrent treatment with temozolomide and radiotherapy followed by maintenance temozolomide is the standard of care for patients with newly diagnosed glioblastoma. Bevacizumab, a humanized monoclonal antibody against vascular endothelial growth factor A, is currently approved for recurrent glioblastoma. Whether the addition of bevacizumab would improve survival among patients with newly diagnosed glioblastoma is not known.
Methods: In this randomized, double-blind, placebo-controlled trial, we treated adults who had centrally confirmed glioblastoma with radiotherapy (60 Gy) and daily temozolomide. Treatment with bevacizumab or placebo began during week 4 of radiotherapy and was continued for up to 12 cycles of maintenance chemotherapy. At disease progression, the assigned treatment was revealed, and bevacizumab therapy could be initiated or continued. The trial was designed to detect a 25% reduction in the risk of death and a 30% reduction in the risk of progression or death, the two coprimary end points, with the addition of bevacizumab.
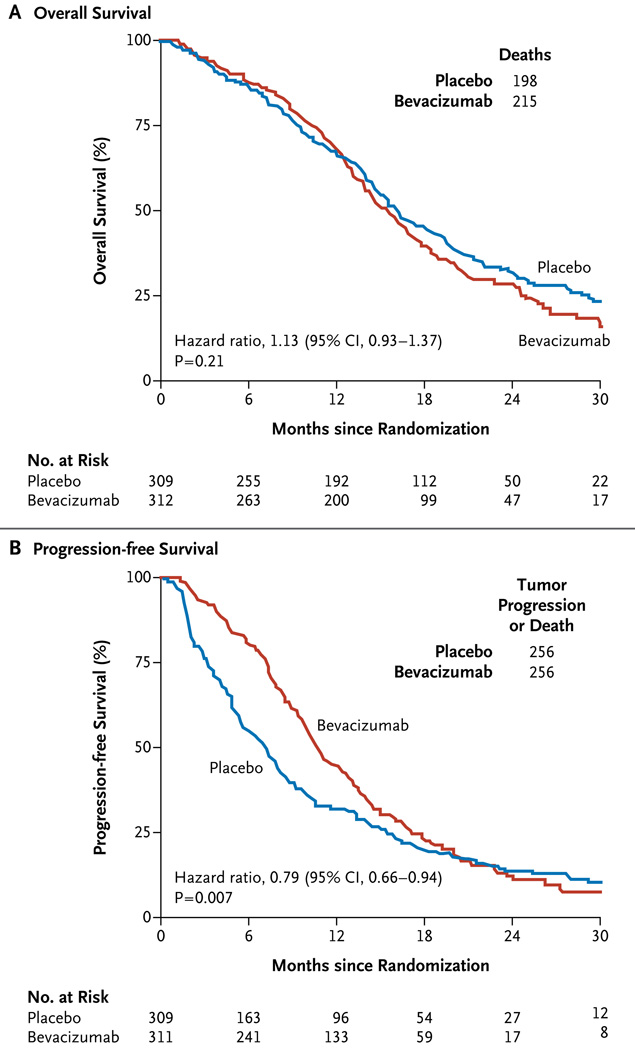
Results: A total of 978 patients were registered, and 637 underwent randomization. There was no significant difference in the duration of overall survival between the bevacizumab group and the placebo group (median, 15.7 and 16.1 months, respectively; hazard ratio for death in the bevacizumab group, 1.13). Progression-free survival was longer in the bevacizumab group (10.7 months vs. 7.3 months; hazard ratio for progression or death, 0.79). There were modest increases in rates of hypertension, thromboembolic events, intestinal perforation, and neutropenia in the bevacizumab group. Over time, an increased symptom burden, a worse quality of life, and a decline in neurocognitive function were more frequent in the bevacizumab group.
Conclusions: First-line use of bevacizumab did not improve overall survival in patients with newly diagnosed glioblastoma. Progression-free survival was prolonged but did not reach the prespecified improvement target. (Funded by the National Cancer Institute; ClinicalTrials.gov number, NCT00884741.).
Figures

Comment in
-
Bevacizumab in glioblastoma--still much to learn.N Engl J Med. 2014 Feb 20;370(8):764-5. doi: 10.1056/NEJMe1313309. N Engl J Med. 2014. PMID: 24552324 No abstract available.
-
Neuro-oncology: Bevacizumab prolongs progression-free survival but not overall survival in newly diagnosed glioblastoma.Nat Rev Neurol. 2014 Apr;10(4):179. doi: 10.1038/nrneurol.2014.47. Epub 2014 Mar 18. Nat Rev Neurol. 2014. PMID: 24638136 No abstract available.
-
Targeted therapies: Further delineating bevacizumab's response spectrum.Nat Rev Clin Oncol. 2014 May;11(5):243-4. doi: 10.1038/nrclinonc.2014.61. Epub 2014 Apr 8. Nat Rev Clin Oncol. 2014. PMID: 24710578 No abstract available.
-
Bevacizumab for newly diagnosed glioblastoma.N Engl J Med. 2014 May 22;370(21):2048-9. doi: 10.1056/NEJMc1403303. N Engl J Med. 2014. PMID: 24849088 No abstract available.
-
Bevacizumab for newly diagnosed glioblastoma.N Engl J Med. 2014 May 22;370(21):2048. doi: 10.1056/NEJMc1403303. N Engl J Med. 2014. PMID: 24849089 No abstract available.
-
Potential novel role of bevacizumab in glioblastoma and cervical cancer.Cancer Biol Ther. 2014 Oct;15(10):1296-8. doi: 10.4161/cbt.29926. Epub 2014 Jul 21. Cancer Biol Ther. 2014. PMID: 25046485 Free PMC article.
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987–996. - PubMed
-
- Lacroix M, Abi-Said D, Fourney DR, et al. A multivariate analysis of 416 patients with glioblastoma multiforme: prognosis, extent of resection, and survival. J Neurosurg. 2001;95:190–198. - PubMed
-
- Stupp R, Hegi ME, Mason WP, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–466. - PubMed
-
- Lund EL, Spang-Thomsen M, Skovgaard-Poulsen H, Kristjansen PE. Tumor angiogenesis — a new therapeutic target in gliomas. Acta Neurol Scand. 1998;97:52–62. - PubMed
-
- Jain RK, di Tomaso E, Duda DG, Loeffler JS, Sorensen AG, Batchelor TT. Angiogenesis in brain tumours. Nat Rev Neurosci. 2007;8:610–622. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical