

Validation of a clinical assessment of spectral-ripple resolution for cochlear implant users
- PMID: 24552679
- PMCID: PMC3999174
- DOI: 10.1097/AUD.0000000000000009
Validation of a clinical assessment of spectral-ripple resolution for cochlear implant users
Abstract
Objectives: Nonspeech psychophysical tests of spectral resolution, such as the spectral-ripple discrimination task, have been shown to correlate with speech-recognition performance in cochlear implant (CI) users. However, these tests are best suited for use in the research laboratory setting and are impractical for clinical use. A test of spectral resolution that is quicker and could more easily be implemented in the clinical setting has been developed. The objectives of this study were (1) To determine whether this new clinical ripple test would yield individual results equivalent to the longer, adaptive version of the ripple-discrimination test; (2) To evaluate test-retest reliability for the clinical ripple measure; and (3) To examine the relationship between clinical ripple performance and monosyllabic word recognition in quiet for a group of CI listeners.
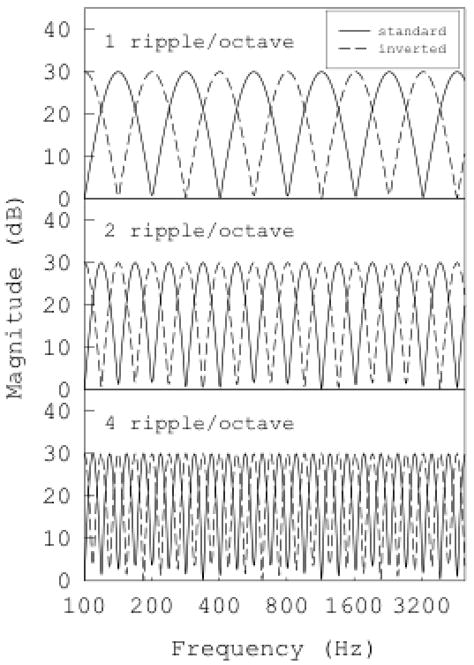
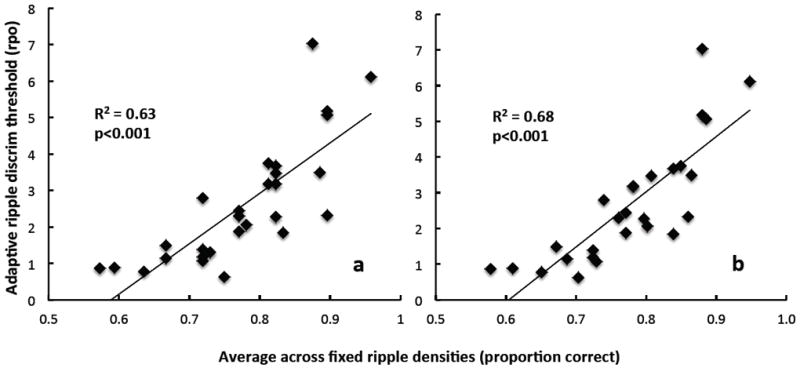
Design: Twenty-eight CI recipients participated in the study. Each subject was tested on both the adaptive and the clinical versions of spectral ripple discrimination, as well as consonant-nucleus-consonant word recognition in quiet. The adaptive version of spectral ripple used a two-up, one-down procedure for determining spectral ripple discrimination threshold. The clinical ripple test used a method of constant stimuli, with trials for each of 12 fixed ripple densities occurring six times in random order. Results from the clinical ripple test (proportion correct) were then compared with ripple-discrimination thresholds (in ripples per octave) from the adaptive test.
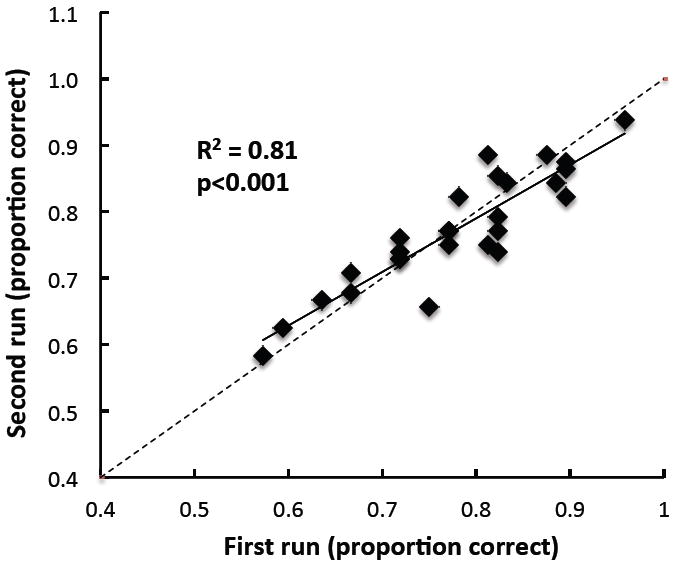
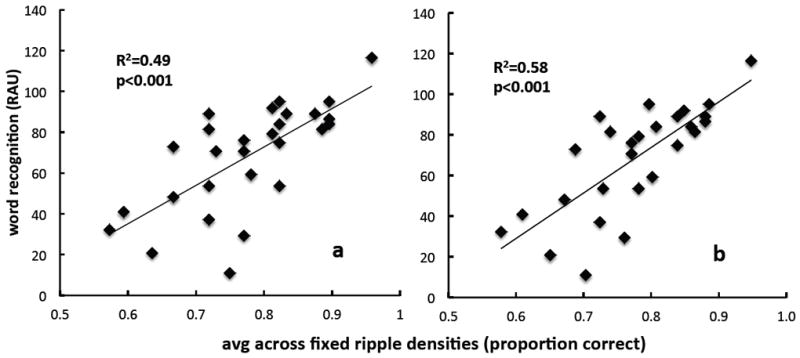
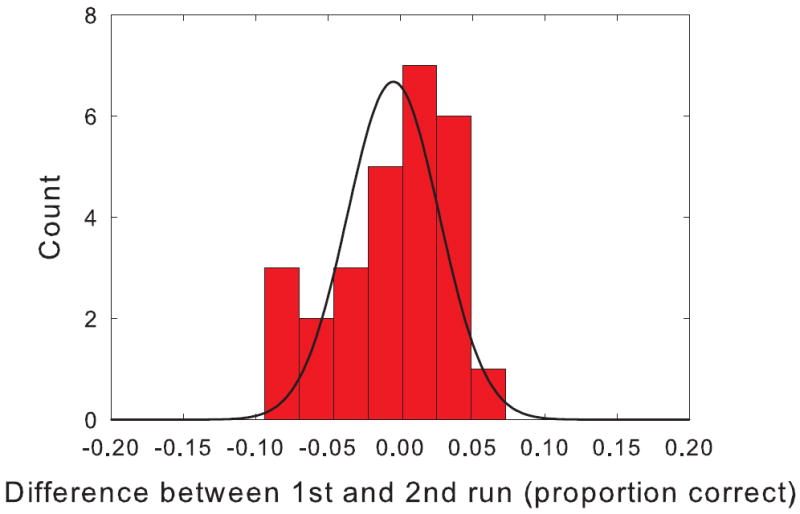
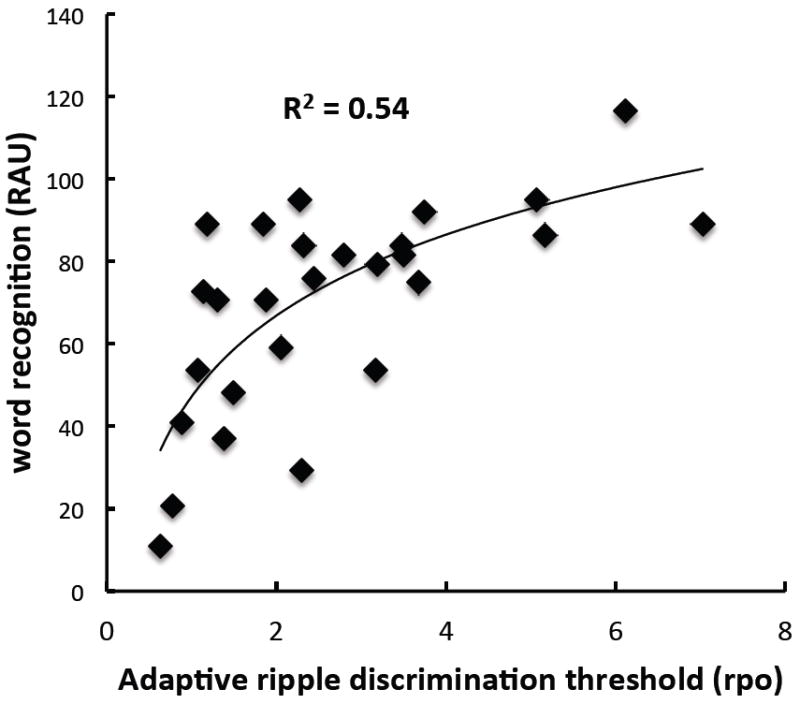
Results: The clinical ripple test showed strong concurrent validity, evidenced by a good correlation between clinical ripple and adaptive ripple results (r = 0.79), as well as a correlation with word recognition (r = 0.7). Excellent test-retest reliability was also demonstrated with a high test-retest correlation (r = 0.9).
Conclusions: The clinical ripple test is a reliable nonlinguistic measure of spectral resolution, optimized for use with CI users in a clinical setting. The test might be useful as a diagnostic tool or as a possible surrogate outcome measure for evaluating treatment effects in hearing.
Conflict of interest statement
Figures
Similar articles
-
Assessment of Spectral and Temporal Resolution in Cochlear Implant Users Using Psychoacoustic Discrimination and Speech Cue Categorization.Ear Hear. 2016 Nov/Dec;37(6):e377-e390. doi: 10.1097/AUD.0000000000000328. Ear Hear. 2016. PMID: 27438871 Free PMC article.
-
Spectral-ripple resolution correlates with speech reception in noise in cochlear implant users.J Assoc Res Otolaryngol. 2007 Sep;8(3):384-92. doi: 10.1007/s10162-007-0085-8. Epub 2007 Jun 21. J Assoc Res Otolaryngol. 2007. PMID: 17587137 Free PMC article.
-
Psychoacoustic abilities associated with music perception in cochlear implant users.Ear Hear. 2010 Dec;31(6):796-805. doi: 10.1097/AUD.0b013e3181e8b7bd. Ear Hear. 2010. PMID: 20595901 Free PMC article.
-
Objective assessment of spectral ripple discrimination in cochlear implant listeners using cortical evoked responses to an oddball paradigm.PLoS One. 2014 Mar 5;9(3):e90044. doi: 10.1371/journal.pone.0090044. eCollection 2014. PLoS One. 2014. PMID: 24599314 Free PMC article.
-
Relationship between behavioral and physiological spectral-ripple discrimination.J Assoc Res Otolaryngol. 2011 Jun;12(3):375-93. doi: 10.1007/s10162-011-0257-4. Epub 2011 Jan 27. J Assoc Res Otolaryngol. 2011. PMID: 21271274 Free PMC article.
Cited by
-
Comparison of the Spectral-Temporally Modulated Ripple Test With the Arizona Biomedical Institute Sentence Test in Cochlear Implant Users.Ear Hear. 2017 Nov/Dec;38(6):760-766. doi: 10.1097/AUD.0000000000000496. Ear Hear. 2017. PMID: 28957975 Free PMC article.
-
Spectrotemporal Modulation Sensitivity in Cochlear-Implant and Normal-Hearing Listeners: Is the Performance Driven by Temporal or Spectral Modulation Sensitivity?Trends Hear. 2020 Jan-Dec;24:2331216520948385. doi: 10.1177/2331216520948385. Trends Hear. 2020. PMID: 32895024 Free PMC article.
-
Cognitive Abilities Contribute to Spectro-Temporal Discrimination in Children Who Are Hard of Hearing.Ear Hear. 2019 May/Jun;40(3):645-650. doi: 10.1097/AUD.0000000000000645. Ear Hear. 2019. PMID: 30130295 Free PMC article.
-
The Characteristics of Adults with Severe Hearing Loss.J Am Acad Audiol. 2018 Sep;29(8):764-779. doi: 10.3766/jaaa.17050. J Am Acad Audiol. 2018. PMID: 30222545 Free PMC article.
-
Frequency detection, frequency discrimination, and spectro-temporal pattern perception in older and younger typically hearing adults.Heliyon. 2023 Aug 6;9(8):e18922. doi: 10.1016/j.heliyon.2023.e18922. eCollection 2023 Aug. Heliyon. 2023. PMID: 37583764 Free PMC article.
References
-
- Berenstein CK, Mens LHM, Mulder JJS, et al. Current steering and current focusing in cochlear implants: comparison of monopolar, tripolar and virtual channel electrode configurations. Ear Hear. 2008;29:250–260. - PubMed
-
- Bernstein LR, Green DM. Detection of simple and complex changes of spectral shape. J Acoust Soc Am. 1987;82 - PubMed
-
- Byrne D, Dillon H, Tran K, et al. An international comparison of long-term average speech spectra. J Acoust Soc Am. 1994;96:2108–2120.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
